Hormones and Fitness

Jorra
Posts: 3,338 Member
Figured I'd start off a discussion into something physiological. Hormones control so much activity in our bodies, what do they do for weight loss, muscle building, or fitness in general?
(Full disclosure: I may have an exam involving the endocrine system soon. :happy:)
(Full disclosure: I may have an exam involving the endocrine system soon. :happy:)
0
Replies
-
Haha - so do I
")
T - 26 hours - I really should be studying
What about T3 or T4 (thyroid hormones) - they should increase BMR ?
The problem with hormones is that they do so many things that supplementation is going to have a LOT of side effects0 -
Oh and of course, if there is any time you are going to have a low carb meal during the day, I recommend dinner
Putting your body into a catabolic state overnight is going to increase your lipolysis, vs a heavy carb meal with the resulting insulin spike will actually make you lipogenic for awhile and waste some of those 8 hrs
I choose free fat burning while you sleep 0
0 -
(Full disclosure: I may have an exam involving the endocrine system soon. :happy:)
AH HA! We're on to you.
Endocrine is pretty damn complicated, to be honest. I'm not sure anyone can really sum it all up as it relates to weight loss, fitness, and muscle mass with 100% accuracy. I work on testosterone and estrogen as it relates to the brain. In very very basic terms, testosterone and estrogen both increase lean body mass (muscle), but testosterone does a better job at it than estrogen, which is part of why men can bulk easier than women. They also regulate bone density, which is why hormone replacement therapy was 'in vogue' for a while for treating osteoporosis. Very simply: They work by virtue of regulating gene transcription. They cue the cell to start making specific proteins, including proteins that form muscle fibers or that regulate the osteoplasts in bone.
Of course... to say that testosterone and/or estrogen alone regulates muscle mass would be simply wrong. Testosterone and estrogen release are controlled by lutenizing hormone and follicle stimulating hormone, which in turn are regulated by other hormones. And then of course you've got growth hormone having its say. And the thyroid hormones coming into play.
Alas, my endocrine is rusty So this is where I bow out.
So this is where I bow out.
I will leave you with this one gem of wisdom: Brains love glucose, testosterone, and estrogen.")
GOOD LUCK! (I'm sure you'll do awesome on your test)0 -
Tardy though I may be to this party, the Cap'n has some info to share!
(As an aside, remember that BMR is not fixed. It moves up or down based on a host of factors, including (perhaps especially) hormonal signaling.)
Nearly all regulation of BMR begins in the hypothalamus. Given that the hypothalamus produces all of the hormones that regulate the pituitary gland AND is the brain center most closely associated with hunger, thirst, satiation, biological clock, etc. It is a target for hormones that affect hunger or metabolism (e.g. cholecystokinin and vasoactive intestinal peptide) AND a producer of hormones that increase or decrease BR. With this in mind, here is a short list of hormone acting through, on, or because of the hypothalamus that regulate BMR.
(1) Somatostatin, Growth hormone releasing hormone (GHRH), and thyrotropin releasing hormone (TRH). These three hormones are produced in the hypothalamus. GHRH targets the somatotrophs of the anterior pituitary gland and leads to the release of growth hormone (GH). TRH targets the thyrotrophs of the anterior pituitary gland and leads to the release of thyroid stimulating hormone (TSH). GH acts directly on some tissues, indirectly on others (through intermediary molecules called insulin-like growth factors) to promote cell growth and metabolism. Given the growth connection, this hormone is a bit more important for metabolism in children than in adults, but is not trivial in adults. TSH, on the other hand, leads to the production of mainly thyroxine (T4) by the thyroid gland follicles. Note that of the monoamine thyroid hormones T3 and T4, T3 is the main actor but T4 is produced in bulk and converted to T3 inside target cells. Thyroxine promotes cellular metabolism in nearly every cell in the body (minus the thyroid itself, brain, spleen, testes, ovaries, and uterus). When it comes to promoting metabolism in the body, thyroxine is the heavy lifter, but note its production is preceded by TRH and TSH. Circling back to somatostatin, it is the OFF hormone for metabolism. It inhibits the production of both GH and TRH, slowing the activity of both of these metabolism stimulating hormones.
(2) Leptin -- Produced by our adipose (fat) tissue, this hormone targets the hypthalamus and increases metabolic rate. Note that the more fat you have the more leptin you produce. Thus, when you have a higher percentage of body fat your hypothalamus is essentially given a signal that says "you have large energy reserves; burn away!" On the other hand, less body fat leads to slower metabolism..."you have less reserve...better slow the burn to conserve!" This is a major reason it is harder to lost the last few pounds because your reduction in body fat creates a sort of metabolic drag.
(3) Digestive Hormones. Many hormones produced by the digestive system to regulate the process of digestion (especially the transition from gastric to intestinal activity) also affect metabolism via their effects on appetite. Cholecystokinin (CCK) which is produced in the duodenum and peptide YY which is produced in both the large and small intestines act as appetite suppressants as the digestive process proceeds and ghrelin which is produced in the stomach when empty and inactive increases appetite. These hormones influence metabolism via their affects on appetite.
(4) Sugar Regulating Hormones. The hormones that regulate blood sugar can potentially influence weight by increasing or decreasing the availability of sugar (glucose) for uptake as an energy source. Insulin gets beaten up here...I hate how people in MFP talk about "evil insulin." If you think insulin is bad, ask someone with T1DM (type I diabetes) about life without insulin. We NEED this hormone to keep our blood sugar in check. The issue with insulin is how much are you producing relative to exercise. If you are highly physically active, even if you gorge on carbs and spike your insulin, you'll see minimal weight gain...skeletal muscle and adipose tissue are the prime targets for insulin and the energy hog that is skeletal muscle will get more of that glucose for ATP synthesis if it is used regularly...weight gain linked to insulin becomes an issue when you are sedentary and your muscle isn't using the sugar...so insulin produces more fat uptake of sugar and energy storage. Bottom line -- insulin is a lovely, lovely hormone and we'd die without it. It creates issues for weight when you mismanage your own body. Note also that many people with T2DM (type II diabetes) end up LOSING weight...blood sugar is high but insulin insensitivity prevents them from accessing that energy, so their body starts relying more on protein and lipid metabolism to survive...hence weight loss.
Two other sugar-regulating hormones bear mention -- insulin's partner, glucagon (also produced by the pancreas) and cortisol (and its fellow glucocorticoids produced in the adrenal cortex). Glucagon increases blood sugar (mainly through causing the liver to release glucose stored as glycogen) as does cortisol (by enhancing non-carbohydrate cellular metabolism). If either of these are produced to excess, the result can be hyperglycemia which in time can lead to increased metabolism (due to extra available fuel) and weight gain.
Cortisol is insidious in that it is linked to stress. A certain amount of cortisol is released every day through a hypothalamus/pituitary pathway (corticotropin releasing hormone (CRH) from the hypothalamus and adrenocorticogropic hormone (ACTH) from the anterior pituitary) to stabilize blood sugar between meals. However, this same pathway can be excessively triggered during stress. When you combine the increased release of cortisol with the (usually) associated release of epinephrine and norepinephrine (adrenaline), the result is a large increase in blood sugar to support the body's stress response, up to and including a full-blown "fight-or-flight" response. The reality is, we evolved to deal with discrete stress...the leopard jumps at us, we run, assuming we survive, it's over. Modern stress is typically more chronic and as such can lead to increases in blood sugar that facilitate the development of both large waistlines and (eventually) T2DM when insulin is overproduced.
On the subject of muscle development, certainly hormones like GH and testosterone facilitate increasing muscle mass, especially during youth and puberty and especially in men. However, real changes in muscle mass are more about usage than hormonal signals and BMR. If we assume the simplified view that there are two basic skeletal muscle fiber types -- slow oxidative and fast glycolytic -- and we understand that muscle is a permanent tissue, so separate from senescence, loss of muscle mass is about atrophy rather than loss of cells, then it's all about exercise. Strength training promotes formation of larger, less durable fast glycolytic fibers. Provided adequate protein is available, strength training (and other anaerobic exercise) facilitates this transformation and mass increases. Endurance training facilitates the conversion of fibers to the slow oxidative type which are much more durable but smaller (containing less protein). Using myself as an example here, I've watched both my fat AND lean body mass drop in recent months...and that isn't a problem. My main form of exercise is running and I do minimal (though now increasing) strength training. Thus, the constant cardio-training has produced more slow fibers in my legs...hence muscle mass decreases as endurance rises. (Skeletal muscle presents the classic trade-off in mechanics...you can't be both highly durable and highly powerful...power sacrifices endurance and endurance sacrifices power.) Since my fitness goals revolve around long-distance running, this is cool with me. (Have you ever seen huge, muscly marathon winners? No! They don't (really can't) exist!) Bottom line -- any hormone that affects growth, blood sugar, or metabolism has the capacity to affect muscle mass, but real changes in muscle mass in adults are a function of exercise before hormones.
Hope this clears some things up! Hit me with any follow up questions you have...I'll be checking in again this evening.
Steve "Cap" Schenk0 -
Endocrine is pretty damn complicated, to be honest.
Ha ha! Missed this before...I tell my students every semester, the two least popular medical specialties are endocrinology and immunology. Who wants to stress over the complexities of these systems when you can make better money with less knowledge as a cardiologist?
(And that's not a knock on cardiologists...they have to know a wholehelluvalot! That just shows how much uglier the complexity of things like the endocrine and immune systems can be!)0 -
Haha - We just finished our Endocrinology block and while the basic principals seem easy, the fact that if you try to draw out an interaction diagram, all you see are lines going everywhere is one reason I am NOT going to be an endocrinologist.
Maybe Cardio 0 -
Ah so! But if you know basic principles in endocrine you can travel many miles with it! That is my approach in class...learn basic principles first, figure out how to apply them, and THEN start working out what specific hormones do.
If anyone is interested, I have some basic flow diagram frameworks for basic relationships (e.g. fundamental BMR regulation, plasma chemistry, blood sugar, reproduction) that I use in my classes that I can share.0 -
That's a pretty awesome bit of info there, Steve. Thanks!
And yes... I'd take cardiology over endocrinology any day :P Or for that matter, I'd take neuroscience over endocrine (which I have). Not that endocrine isn't interesting... just that you think you've got it only to find out that you really don't. It's not just hormone goes up, hormone goes down... /sigh
But I totally agree about learning basic principles first. You can get some good milage out of the basics.
Flow diagrams, huh? I like diagrams. Especially if they're colored I'd love to see a diagram or three. 0 -
Esp Repro - next block on the list 0
-
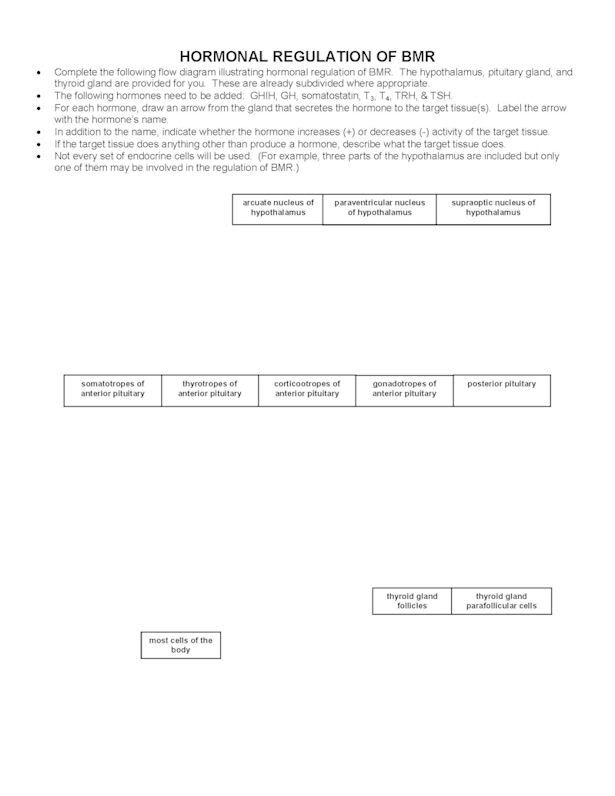
Here is a sample flow diagram framework I use in class. It's not in color/no bells/no whistles. It's designed for students to sit in groups of 3 - 5 and, based on reading assignments, diagram all hormones linked to a particular process. This one is for the hypothalamic/pituitary axis and BMR.
 0
0 -
over 17 yrs since I've had any active interactions with these terms so please forgive my errors:
Glycogenisis: Specifically Liver response to hard exercise and the resulting sugar flood + type 2 diabetes. I know that HIIT and Strength training both activate muscle growth and burn visceral fat better than other types. I also know that you get a big glucose spike after hard exercise. Without excersise I seem to experience a "push" at night and wake up with high fasting BG. usually in the 125-135 range. If I excersise in the morning or at lunch (doesn't matter the routine intensity) I still have high BG. However, I've noticed if I strength train with heavy weights in the evening, when I get up my BG is in the 100-118 range. I'm also pretty consistantly STARVING on my recovery day.
So am I using the correct strategy for exercise time?
I'm down to 5 units of lantus on non-workout nights, so what do you think strategy wise? Byetta really helped but I can no longer afford it. OH and "Evil Insulin"???!!!! wtf!? More like evil Triglycerides and evil Uric Acid! Sheesh!0 -
Ok, something I remembered from Dr Oz ages ago (ugh, I don't really like him, but whatever :P)
Ghrelin? Does this exist and does it really regulate hunger levels?
I have not seen it brought up on these forums before, and admittedly never looked into it myself.0 -
Speaking of hormones, ninerbuff just brought up a fantastic point in an HCG thread.
How can people claim that HCG reduces hunger when it's a pregnancy hormone and pregnant women are not necessarily lacking in hunger...0 -
zactly. The only hunger abatement you get is when the baby is so big that your stomach is compressed and there's no physical room for food! Not to mention there's not one study that didn't result in the same amount of weight loss with a placebo and no it doesn't matter if it's injected or not. same results!0
-
Ok, something I remembered from Dr Oz ages ago (ugh, I don't really like him, but whatever :P)
Ghrelin? Does this exist and does it really regulate hunger levels?
I have not seen it brought up on these forums before, and admittedly never looked into it myself.
Ghrelin does regulate hunger - along with a lot of other things. It is produced in the stomach and basically acts as a appetite stimulant. The main counter regulatory hormone for this is leptin, produced in the adipose tissue that acts as an appetite suppresant.
Leptin is thought to be linked to obesity - Obese individuals are thought to become leptin resistant (think of it as analagous to insulin resistance - though they have an excess of leptin in their blood stream, they do not respond to it)
With ghrelin however, the link is more tenuous - studies have shown that obese individuals actually have decreased circulating ghrelin, suggesting it is not as important a player. Ghrelin also performs many other important functions in the body, including acting as an anti-inflammatory, as well as being a potent stimulator of other hormones, including growth hormone. Basically, like insulin - its not really a 'bad hormone' - there is no such thing. It just is 0




This discussion has been closed.