Cholesterol and Mortality (Higher is Better)

FIT_Goat
Posts: 4,227 Member
Ran across this today.
http://healthimpactnews.com/2015/japanese-research-exposes-statin-scam-people-with-high-cholesterol-live-longer/
Pretty interesting read, especially for those who are still worried about this diet's effect on cholesterol levels.
http://healthimpactnews.com/2015/japanese-research-exposes-statin-scam-people-with-high-cholesterol-live-longer/
Pretty interesting read, especially for those who are still worried about this diet's effect on cholesterol levels.
0
Replies
-
Interesting!
DH has low cholesterol, super-low HDL (so his ratio is bad) and coronary artery disease. One of our 6y/o twins seems to have inherited the same profile. I need to get these two eating more fat! (Or at least the kid. DH's cardiologist would not approve. Sigh. I would love to find more research on patients with existing CAD, and stents, eating LCHF.)0 -
A news report of a blog report of an article?
Here's the blog:
http://drmalcolmkendrick.org/2015/05/18/hats-off-to-the-japanese/
And here's the article:
https://www.karger.com/Article/Abstract/381654
The lowest mortality rate for men was associated with LDL between 120-139 mg/dl. Mortality went up on both the low end and high end.
For total cholesterol, mortality for men was lowest between 200-230 mmol/l.
0 -
A news report of a blog report of an article?
Here's the blog:
http://drmalcolmkendrick.org/2015/05/18/hats-off-to-the-japanese/
And here's the article:
https://www.karger.com/Article/Abstract/381654
The lowest mortality rate for men was associated with LDL between 120-139 mg/dl. Mortality went up on both the low end and high end.
For total cholesterol, mortality for men was lowest between 200-230 mmol/l.
Ash Simmonds has some good stuff on that mortality curve. Where overall mortality over several studies tends to be lowest between around 200 and 240.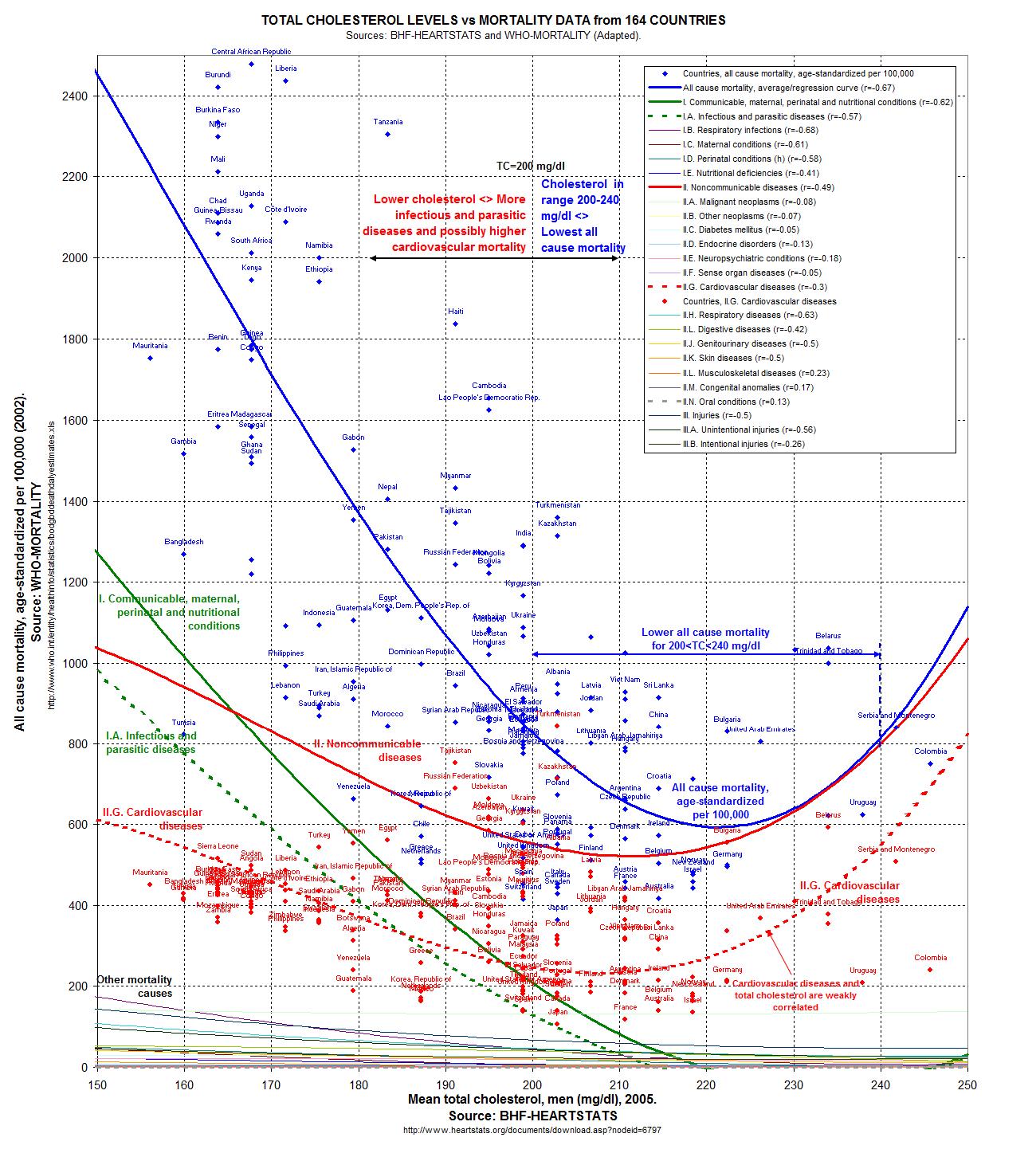
As for which link I turned up, it was the one which was shared on my newsfeed this morning and also had the links for the videos (which are interesting in their own right).0 -
I've read some of Malcolm Kendrick's stuff. I even have his latest book checked out from the library (but haven't read it yet). The gist of his message seems to be that looking at relative risk makes the absolute risk seem overblown.
High LDL does seem to be a significant risk at the highest levels, but not at the levels normally recommended for treatment.
Total cholesterol just has too many confounders mixed in, so almost nobody pays attention to it anymore, but even your graph shows risk increases at higher levels.
The Japanese study sited in the article in the OP shows modest increase in all-cause mortality, but the increased risk for CHD mortality was more significant.
So what can we take from all of this?
Cholesterol does seem to help the immune system, so that may be why all-cause mortality doesn't increase much with higher levels.
It is a factor in CHD, and the mechanism is sort of known, but it's complex, and inflammation is a big factor as well.
If your LDL is off-the-charts high, that's a valid reason to worry.
If your LDL is mildly high, get your inflammation markers checked, like CRP.
In terms of mechanisms of plaque formation, this article is pretty good:
http://www.scientificamerican.com/article/atherosclerosis-the-new-view/0 -
I think we're both agreeing on the same thing. Maybe you're not comfortable with the statement that "Higher is better" or something. The cholesterol worry is vastly overblown and the people with cholesterol in the range associated with best mortality are told their cholesterol is too high and needs to be fixed.0
-
Yeah, I think the risk is overblown and statins are prescribed too aggressively.
But it's a hot-button for me since the only reason I went low-carb was to reduce CHD risk. Most of my risk markers improved except for LDL concentration.
I'm at the age where I have to worry about this stuff. You have a few more years before it's a concern.
Interestingly, my risk of death by cancer seems to go down starting about now. CHD is my main concern from here on out..png) 0
0 -
Thanks everyone for providing this really great info. One downside is the first video link lead me to 5 others.
") 0
0 -
I just read Kendrick's book, The Great Cholesterol Con. It said the same thing. High cholesterol has almost no realtioship with CAD. The exception he mentions is men under age 50 who have very high cholesterol levels. He even points out that women over 50 tend to develop a higher risk of CAD if you lower their cholesterol. They do better with higher cholesterol.
About the only "cholesterol" I worry about is triglycerides as higher levels can match higher levels of CAD risk (not a cause though). I also spare a thoug for Lp (a) because that can also correlate to CAD risk and mine was a bit high a couple of years back.
As far as I'm concerned, who cares if cholesterol is high for me because it has absolutely no dangers for me. It's like saying I have a greater risk of CAD if I grow I mustache just because peri/post menopausal women tend to grow mustaches around the same time that CAD could start showing up. I'm not really fussed about it.
The only reason I like seeing "improved" cholesterol numbers in low carbers is because that is often a worry for people against trying it. It is easier to say "See? LCHF improves cholesterol" than "Cholesterol improved but it doesn't matter anyways". Most people that I know won't believe it.
Kendrick's theory is that stress causes CAD. Seems over simplified to me. I do think cholesterol is just a marker of poor health that means you could develop CAD, I don't beleieve it is the cause.0 -
I'm looking forward to reading his book, but most of the stuff I've read from him focuses on epidemiological studies. Those are great for forming hypotheses, but that's about it.
Once you move beyond epidemiology, there's good evidence that LDL plays a role in heart disease.
For one thing, when they look at the mechanism of plaque formation, LDL in the arterial wall starts the process.
They also look at people with genetic mutations. Those with mutations that cause high LDL have high rates of heart disease, and those with mutations that cause low LDL have lower rates of heart disease.
The most recent drug target is PCSK9 because people with PCSK9 mutations (and low LDL) have about 1/2 the risk of heart disease as those without the mutation.
So LDL is definitely a factor. It's not the only factor, and there's no clearly optimal level yet.
I still haven't seen any long-term studies of low-carb diets and heart disease -- just short-term studies and risk factors.0 -
I'm looking forward to reading his book, but most of the stuff I've read from him focuses on epidemiological studies. Those are great for forming hypotheses, but that's about it.
Once you move beyond epidemiology, there's good evidence that LDL plays a role in heart disease.
For one thing, when they look at the mechanism of plaque formation, LDL in the arterial wall starts the process.
They also look at people with genetic mutations. Those with mutations that cause high LDL have high rates of heart disease, and those with mutations that cause low LDL have lower rates of heart disease.
The most recent drug target is PCSK9 because people with PCSK9 mutations (and low LDL) have about 1/2 the risk of heart disease as those without the mutation.
So LDL is definitely a factor. It's not the only factor, and there's no clearly optimal level yet.
I still haven't seen any long-term studies of low-carb diets and heart disease -- just short-term studies and risk factors.
Bleh, I think you are mixing up info on the PCSK9 mutations...those with mutations have homozygous familial hypercholesterolemia, over expressing PCSK9 & degrading LDL-Receptors too easily. Less LDL-Receptors = more serum LDL-C. The OTHER drug target with mutations involved Cholesterol Ester Transferase (CETP)-inhibitors; persons with these mutations lacked Cholesterol Ester Transferase, thus had abnormally high HDL & longer longevity. Ultimately, CETP-inhibition as a drug target has been abandoned due to increased risk in cardiovascular mortality...hypothesized to be due to an increase in the wrong subtype of HDL, not associated with increased cardiovascular protection.0 -
Good timing for me on this! I live in Japan, where they use the guidelines the article mentions:
Indeed, the major portion of this supplementary issue (from Chapter 4 onward) is given over to our detailed examination and critique of guidelines published by the Japan Atherosclerosis Society. We dedicate a large portion of this work to these guidelines because they are generally held in high regard in Japan, and the country’s public health administration mechanism complies with them without question. - See more at: http://healthimpactnews.com/2015/japanese-research-exposes-statin-scam-people-with-high-cholesterol-live-longer/#sthash.TeGpP5Ra.dpuf
My health check results just came back (in Japanese but have figured out how to translate them) from the blood test in May this year, and it shows my total chol went up to 230 (from 221 six months earlier), but my HDL-C was 87 (no change), LDL-C was 133 (up from 113), trigs were down to 44 (from 59)--and so the trig/HDL ratio was 0.51 (down from 0.67)! That is my best yet, but they dropped my rating from "A2" last time to "B1." There is an asterisk beside the total chol number... trying to scare me. Worried me for a bit, but now am feeling reassured again.
Thanks for the link -- will be reading the original. 3 of my 4 siblings are all on statins. Mom died of heart attack/strokes. But Dad lived to 95! So who knows.0 -
I'm looking forward to reading his book, but most of the stuff I've read from him focuses on epidemiological studies. Those are great for forming hypotheses, but that's about it.
Once you move beyond epidemiology, there's good evidence that LDL plays a role in heart disease.
For one thing, when they look at the mechanism of plaque formation, LDL in the arterial wall starts the process.
They also look at people with genetic mutations. Those with mutations that cause high LDL have high rates of heart disease, and those with mutations that cause low LDL have lower rates of heart disease.
The most recent drug target is PCSK9 because people with PCSK9 mutations (and low LDL) have about 1/2 the risk of heart disease as those without the mutation.
So LDL is definitely a factor. It's not the only factor, and there's no clearly optimal level yet.
I still haven't seen any long-term studies of low-carb diets and heart disease -- just short-term studies and risk factors.
Bleh, I think you are mixing up info on the PCSK9 mutations...those with mutations have homozygous familial hypercholesterolemia, over expressing PCSK9 & degrading LDL-Receptors too easily.
There appear to be multiple mutations. A couple are associated with FH. But I was referring to this one:
http://sitn.hms.harvard.edu/flash/2015/a-potential-new-weapon-against-heart-disease-pcsk9-inhibitors/
Inactivated PCSK9 decreases LDL so much that one rare individual with two inactive copies of PCSK9 has LDL levels of 14! [3,8-9]. Researchers then examined a long-term study of heart disease risk to compare risk in participants with and without these inactivating mutations. Not only was an inactivating PCSK9 mutation associated with a 15-28% reduction in LDL, but these patients also had a whopping 47-88% reduction in heart disease risk [3,10]. In addition, their very low cholesterol levels do not appear to cause any negative effects elsewhere in the body. This study, published in 2006 in the New England Journal of Medicine, cemented the status of PCSK9 as a very attractive and potentially lucrative drug target.0 -
I'm looking forward to reading his book, but most of the stuff I've read from him focuses on epidemiological studies. Those are great for forming hypotheses, but that's about it.
Once you move beyond epidemiology, there's good evidence that LDL plays a role in heart disease.
For one thing, when they look at the mechanism of plaque formation, LDL in the arterial wall starts the process.
They also look at people with genetic mutations. Those with mutations that cause high LDL have high rates of heart disease, and those with mutations that cause low LDL have lower rates of heart disease.
The most recent drug target is PCSK9 because people with PCSK9 mutations (and low LDL) have about 1/2 the risk of heart disease as those without the mutation.
So LDL is definitely a factor. It's not the only factor, and there's no clearly optimal level yet.
I still haven't seen any long-term studies of low-carb diets and heart disease -- just short-term studies and risk factors.
LDL definitely plays a role in CAD but I don't think it is a cause. It seems like more of a tool that is used by the body in that unhealthy situation. Lowering LDL is sort of like taking away most of the nails when someone is trying to build an unsound and not safe structure. More nails will usually be found, but the nails aren't the main problem.
All that being said, if I had high LDL and my doctor was concerned and wanted to treat it, I would probably have a hard time walking away from that.0 -
Right. I view drugs that lower LDL as using a sledgehammer to fix a watch. Few docs look at treating the cause -- just relieving the symptoms (and creating new ones).
But high LDL is a risk factor. And LDL goes up on a low-carb diet. I'm sticking with low-carb, though. Other risk factors go down, and I'm guessing that inflammation goes down as well. Perhaps less LDL is oxidized and fewer plaques are formed.
It would be nice to know that for sure. I'd love to see a study that shows low-carb reduces plaque formation, or better yet, that plaques regress on low-carb.
Anybody want to do that study? 0 -
@wabmester there are some studies that I have read about how in combination Vit D3/Vit K2 can reverse plaque formations that contain calcium. After being stuck with my Vit D levels in the 20's for years this year I learned about the importance of Vit K2 and got my Vit D levels into the 90's range I guess for the first time in my life. 70-90 levels are reported by some to be preventive against and may help cure cancer. I have seen no hard research that supports that. My direct concern is managing autoimmune disease related pain.
Low levels of Vit K2 is thought to deposit calcium in the arteries, kidneys, etc. Vit K2 is required to tell Vit D where to deposit the calcium or something like that the best I remember. You can google the subject and find a lot to read.
Since Low Carb High Fat as cut my pain that means it has cut my body's level of inflammation I would think. We know systemic inflammation is key to plaques forming.0 -
My impression is that calcified plaques are stable plaques, and it's the unstable plaques that pose the biggest risk.
But I guess I shy away from supplements on a philosophical basis. The high rate of heart disease seems to be a relatively recent phenomenon. So that suggests to me that some relatively recent change in our diet or other environmental factor is probably the cause.
It may be as simple as the increase in refined carbs. But maybe the types of fats we're eating now is also a factor. I'd love to know the answer. 0 -
@wabmester I encourage you to think of supplements on a physiological basis rather than on a philosophical basis.
There is research shows taking a calcium supplement may increased risk of heart disease by 24%. Now research shows this may be due to a lack of Vitamin D and Vitamin K2.
I now take Vit K2 to prevent against heart disease and liver cancer. I take Vit D3 to protect against premature death from all causes. Keep in mind I only learned about Vit K2 this year and still have much to learn.
Dr. William Davis wrote the article below before he wrote Wheat Belly.
lifeextension.com/magazine/2008/3/Protecting-Bone-And-Arterial-Health-With-Vitamin-K2/Page-010






This discussion has been closed.