Welcome to Debate Club! Please be aware that this is a space for respectful debate, and that your ideas will be challenged here. Please remember to critique the argument, not the author.
How do we judge a healthy weight range? BMI is no longer valid?
Replies
-
CipherZero wrote: »BMI is useful for population studies because it requires two static measurements that anyone with three brain cells can take; trying to apply BMI to individuals without any other contextual information is silliness at best.
When I was at a "proper" weight that fit BMI, I was considerably weaker both in raw numbers and proportional ones. Once I stopped caring about BMI, my weight went up slightly (about 10%) and my strength rocketed up 20% and is still rising while my body weight remains steady.
I weighed in at 184.6 as of this morning, which is where I've been for six months. My BMI is 28.9. My "ideal body weight", depending on the formula used, is between 144lbs and 147 lbs. I also have a combined squat, bench press, and deadlift that puts me in the top 4000 people in the drug-drug-tested IPF power lifting federation, and carry about 22-24% body fat.
My blood work is nearly perfect, aside from known genetic faults. I can work harder and longer than work colleagues half my age. All of my doctors agree I should keep doing what I'm doing because it's clearly working.
The tl;dr: BMI is a stupid measure for fit people.
[note: all edits were for typos]
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.1 -
coreyreichle wrote: »
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.
Based on my Wilks score comparison from the collected results of IPF meets as found at http://www.openpowerlifting.org/ - it's not just something I'm pulling out of my *kitten*. My avatar isn't just for show.
Squat's at 1.5, bench is over bodyweight, and my deadlift is lagging behind 2x body weight, but I'mma still trying.
I'll put my money where my mouth is - here's the last six months of logs.
Finally, comparing my claims to those made by that *kitten* is a personal insult I'd rather not hear again.1 -
There are two parts to "BMI". There's the math, and there's the judgment that people infer from the "range" they fall into. The math is the simple part that results in a number like "32.1" or "24". No one has a problem with this part it seems.
What people seem to have a problem with is the judgment they assign to themselves when they see something other than "Normal". This of course makes it "invalid" and "outdated".
Well, OK, go ahead. Screw with the ranges all you want until all of you delicate snowflakes can call yourselves normal. But don't come crying to me when that "size 8" article of clothing you bought is now large enough to use for a 12 man camping excursion. You brought this madness on yourselves.
I have a problem with the math.1 -
coreyreichle wrote: »CipherZero wrote: »BMI is useful for population studies because it requires two static measurements that anyone with three brain cells can take; trying to apply BMI to individuals without any other contextual information is silliness at best.
When I was at a "proper" weight that fit BMI, I was considerably weaker both in raw numbers and proportional ones. Once I stopped caring about BMI, my weight went up slightly (about 10%) and my strength rocketed up 20% and is still rising while my body weight remains steady.
I weighed in at 184.6 as of this morning, which is where I've been for six months. My BMI is 28.9. My "ideal body weight", depending on the formula used, is between 144lbs and 147 lbs. I also have a combined squat, bench press, and deadlift that puts me in the top 4000 people in the drug-drug-tested IPF power lifting federation, and carry about 22-24% body fat.
My blood work is nearly perfect, aside from known genetic faults. I can work harder and longer than work colleagues half my age. All of my doctors agree I should keep doing what I'm doing because it's clearly working.
The tl;dr: BMI is a stupid measure for fit people.
[note: all edits were for typos]
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.
You can't be serious for that being "above average". Jesus Christ people are weak. I hit 2.25x on deads, 1.75x on squat, 0.8x on OHP, and 1.25x on bench a month in. :-/-1 -
Gallowmere1984 wrote: »coreyreichle wrote: »CipherZero wrote: »BMI is useful for population studies because it requires two static measurements that anyone with three brain cells can take; trying to apply BMI to individuals without any other contextual information is silliness at best.
When I was at a "proper" weight that fit BMI, I was considerably weaker both in raw numbers and proportional ones. Once I stopped caring about BMI, my weight went up slightly (about 10%) and my strength rocketed up 20% and is still rising while my body weight remains steady.
I weighed in at 184.6 as of this morning, which is where I've been for six months. My BMI is 28.9. My "ideal body weight", depending on the formula used, is between 144lbs and 147 lbs. I also have a combined squat, bench press, and deadlift that puts me in the top 4000 people in the drug-drug-tested IPF power lifting federation, and carry about 22-24% body fat.
My blood work is nearly perfect, aside from known genetic faults. I can work harder and longer than work colleagues half my age. All of my doctors agree I should keep doing what I'm doing because it's clearly working.
The tl;dr: BMI is a stupid measure for fit people.
[note: all edits were for typos]
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.
You can't be serious for that being "above average". Jesus Christ people are weak. I hit 2.25x on deads, 1.75x on squat, 0.8x on OHP, and 1.25x on bench a month in. :-/
:goldstarforyou:3 -
Gallowmere1984 wrote: »coreyreichle wrote: »CipherZero wrote: »BMI is useful for population studies because it requires two static measurements that anyone with three brain cells can take; trying to apply BMI to individuals without any other contextual information is silliness at best.
When I was at a "proper" weight that fit BMI, I was considerably weaker both in raw numbers and proportional ones. Once I stopped caring about BMI, my weight went up slightly (about 10%) and my strength rocketed up 20% and is still rising while my body weight remains steady.
I weighed in at 184.6 as of this morning, which is where I've been for six months. My BMI is 28.9. My "ideal body weight", depending on the formula used, is between 144lbs and 147 lbs. I also have a combined squat, bench press, and deadlift that puts me in the top 4000 people in the drug-drug-tested IPF power lifting federation, and carry about 22-24% body fat.
My blood work is nearly perfect, aside from known genetic faults. I can work harder and longer than work colleagues half my age. All of my doctors agree I should keep doing what I'm doing because it's clearly working.
The tl;dr: BMI is a stupid measure for fit people.
[note: all edits were for typos]
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.
You can't be serious for that being "above average". Jesus Christ people are weak. I hit 2.25x on deads, 1.75x on squat, 0.8x on OHP, and 1.25x on bench a month in. :-/
I'm going based on general guidelines. Those are what put you above average in muscle strength.0 -
CipherZero wrote: »coreyreichle wrote: »
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.
Based on my Wilks score comparison from the collected results of IPF meets as found at http://www.openpowerlifting.org/ - it's not just something I'm pulling out of my *kitten*. My avatar isn't just for show.
Squat's at 1.5, bench is over bodyweight, and my deadlift is lagging behind 2x body weight, but I'mma still trying.
I'll put my money where my mouth is - here's the last six months of logs.
Finally, comparing my claims to those made by that *kitten* is a personal insult I'd rather not hear again.
So, since you squat puts you at about "normal" for strength, under on your deads, I'm going to assume you're not a special snowflake, and the BMI fits you just fine.0 -
Packerjohn wrote: »A 275 pound 5'5" individual wants to lose weight. Don't you think the BMI calculation will provide them with a reasonable range to shoot for in the vast majority of cases? If you don't think it is what, that is widely available at low cost, would be better? Do you think it would yield a significantly different result than BMI for most people?
A mirror.")
3 -
amusedmonkey wrote: »BMI is a good general indicator. Slightly under or slightly over the normal range is fine. Is your weight within the normal BMI range or close to it? Is your natural waist circumference 80 cm (~31.5 inches) or under? Are you pleased with the way you look?
If the answer is yes to the above, you are safely within a good range. Are your general health markers within a good range (blood sugar, cholesterol..etc)? If they are not, you may find being at the lower end of BMI more beneficial.
BMI is not invalid, it's just more valid for some than others. Normal weight is defined as a range not a number for a reason, to accommodate some of that variance among people. Some are still outliers, but not as many as you think and not as many women. For those who are, being at 27 or 17 BMI, for example, and healthy otherwise is a nonissue.
I'm curious where the 31.5" waist thing is coming from. I'm 5'8", normal BMI, waist is 34".
Several studies found that abdominal obesity, even within normal BMI, carries higher risks for things like type 2 diabetes and cardiovascular disease and that cut off point where risk factors start to climb up was pinpointed at 80 cm for women. You may find this article helpful as it includes links to several studies:
https://www.hsph.harvard.edu/obesity-prevention-source/obesity-definition/abdominal-obesity/3 -
amusedmonkey wrote: »
Several studies found that abdominal obesity, even within normal BMI, carries higher risks for things like type 2 diabetes and cardiovascular disease and that cut off point where risk factors start to climb up was pinpointed at 80 cm for women. You may find this article helpful as it includes links to several studies:
https://www.hsph.harvard.edu/obesity-prevention-source/obesity-definition/abdominal-obesity/
^^^^This!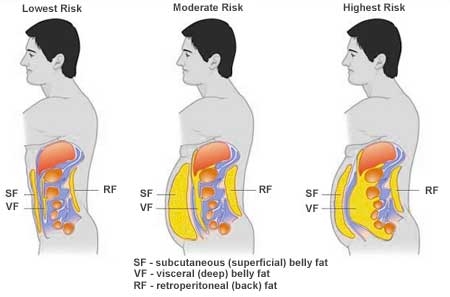
We all have the ability to lower our risk. Who wouldn't want to do that and shoot for the lowest risk picture on the left?
2 -
coreyreichle wrote: »CipherZero wrote: »coreyreichle wrote: »
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.
Based on my Wilks score comparison from the collected results of IPF meets as found at http://www.openpowerlifting.org/ - it's not just something I'm pulling out of my *kitten*. My avatar isn't just for show.
Squat's at 1.5, bench is over bodyweight, and my deadlift is lagging behind 2x body weight, but I'mma still trying.
I'll put my money where my mouth is - here's the last six months of logs.
Finally, comparing my claims to those made by that *kitten* is a personal insult I'd rather not hear again.
So, since you squat puts you at about "normal" for strength, under on your deads, I'm going to assume you're not a special snowflake, and the BMI fits you just fine.
You're letting him distract you with his strength numbers. Remember his 22-24% body fat?
He can post all the stats he wants about his lifting, but the body fat says it all.8 -
GottaBurnEmAll wrote: »coreyreichle wrote: »CipherZero wrote: »coreyreichle wrote: »
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.
Based on my Wilks score comparison from the collected results of IPF meets as found at http://www.openpowerlifting.org/ - it's not just something I'm pulling out of my *kitten*. My avatar isn't just for show.
Squat's at 1.5, bench is over bodyweight, and my deadlift is lagging behind 2x body weight, but I'mma still trying.
I'll put my money where my mouth is - here's the last six months of logs.
Finally, comparing my claims to those made by that *kitten* is a personal insult I'd rather not hear again.
So, since you squat puts you at about "normal" for strength, under on your deads, I'm going to assume you're not a special snowflake, and the BMI fits you just fine.
You're letting him distract you with his strength numbers. Remember his 22-24% body fat?
He can post all the stats he wants about his lifting, but the body fat says it all.
Well, there's that too... :P0 -
Gallowmere1984 wrote: »coreyreichle wrote: »CipherZero wrote: »BMI is useful for population studies because it requires two static measurements that anyone with three brain cells can take; trying to apply BMI to individuals without any other contextual information is silliness at best.
When I was at a "proper" weight that fit BMI, I was considerably weaker both in raw numbers and proportional ones. Once I stopped caring about BMI, my weight went up slightly (about 10%) and my strength rocketed up 20% and is still rising while my body weight remains steady.
I weighed in at 184.6 as of this morning, which is where I've been for six months. My BMI is 28.9. My "ideal body weight", depending on the formula used, is between 144lbs and 147 lbs. I also have a combined squat, bench press, and deadlift that puts me in the top 4000 people in the drug-drug-tested IPF power lifting federation, and carry about 22-24% body fat.
My blood work is nearly perfect, aside from known genetic faults. I can work harder and longer than work colleagues half my age. All of my doctors agree I should keep doing what I'm doing because it's clearly working.
The tl;dr: BMI is a stupid measure for fit people.
[note: all edits were for typos]
So, we can assume you deadlift more than 2x your body weight, bench more than 1.5x your body weight, and squat more than 1.5x your body weight? Because your "top 4000 people" sounds a whole lot like Ragen Chastain's claims of being an uber-athlete.
Because that would put you "above average" for fitness, if you use those measures.
You can't be serious for that being "above average". Jesus Christ people are weak. I hit 2.25x on deads, 1.75x on squat, 0.8x on OHP, and 1.25x on bench a month in. :-/
You are something special1 -
roamingtiger wrote: »Not sure. BMI says I'm obese haha
Reported BMI for bullying6 -
...
The thing to keep in mind: it is a guideline, and BMI gives a very generous range regarding what is considered a healthy weight. (My healthy weight range is defined as between 111-149 lbs- that's almost 40 lbs of wiggle room!) The problem is, there's been a movement of people in overweight nations that are unhappy with the healthy weight ranges given and have been trying to denounce the whole thing as bogus....
My BMI says i should weigh between 98-119 lbs. that's NOT ever going to happen, unless i quit eating all together and only drink water and exercise hours/day, every day. Therefore, IMHO, the BMI chart is useless for the majority of people. the last time i weighed ANYWHERE near 119 was in High School, YEARS ago.0










This discussion has been closed.
Categories
- All Categories
- 1.4M Health, Wellness and Goals
- 396.9K Introduce Yourself
- 44.2K Getting Started
- 260.9K Health and Weight Loss
- 176.3K Food and Nutrition
- 47.6K Recipes
- 232.8K Fitness and Exercise
- 454 Sleep, Mindfulness and Overall Wellness
- 6.5K Goal: Maintaining Weight
- 8.7K Goal: Gaining Weight and Body Building
- 153.3K Motivation and Support
- 8.3K Challenges
- 1.3K Debate Club
- 96.5K Chit-Chat
- 2.6K Fun and Games
- 4.5K MyFitnessPal Information
- 16 News and Announcements
- 18 MyFitnessPal Academy
- 1.4K Feature Suggestions and Ideas
- 3.1K MyFitnessPal Tech Support Questions