Welcome to Debate Club! Please be aware that this is a space for respectful debate, and that your ideas will be challenged here. Please remember to critique the argument, not the author.
New study suggests exercise may play more important role in weight loss
Replies
-
Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »
And they explained who the underrepresented in the study were:EvgeniZyntx wrote: »Traveler120 wrote: »
I don't know where you're trying to go with this. I think the part you should have bolded was this one:EvgeniZyntx wrote: »Traveler120 wrote: »Gianfranco_R wrote: »Traveler120 wrote: »
Even from your graph, the widest point of variation is 1375 and 1475. That's only 100 calories. I don't know where you're getting 200 or more from your graph.EvgeniZyntx wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »Exercise is extremely important when in a calorie deficitbecause without it you can actually lower the rate you use calories while resting. This was proven by a U.S.government study done in 2009. Ci/co works but what good is losing the weight if you're just going to put it back on because you are no longer burning the same amount of calories at rest as you were before you lost the weight?
https://www.nia.nih.gov/newsroom/announcements/2009/05/study-shows-metabolic-adaptation-calorie-restriction
May I ask how long you've been in maintenance? 3 years into maintenance here, and I didn't exercise at all during my weight loss phase. My TDEE is spot on and has been since I started this whole thing back in 2012.
If you look at my profile it is obvious that I am not into maintenance "here." I did however lose 38 pounds about 28 years ago from diet and exercise and did a pretty good job of maintaining it until about 7 years ago. That would put me in maintenance for about 21 years. Of course that was before MFP. Exercise is important during weight loss to preserve our bone mass and metabolism as we get older. If you're happy and your TDEE is spot on then I'm happy for you. Not everyone is as lucky.
Yes, people keep telling my I'm a lucky freak of nature special snowflake TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
These formulas are very rough estimators - here is an example graph of two leading formulas. If you find them accurate it is just confirmation bias. In every study they only correspond to about 65% of metabolic factors.
For example, consider women weighing 75Kg of different heights, you'll see that the equations only match at one point and may differ as much as 200 cals (or more).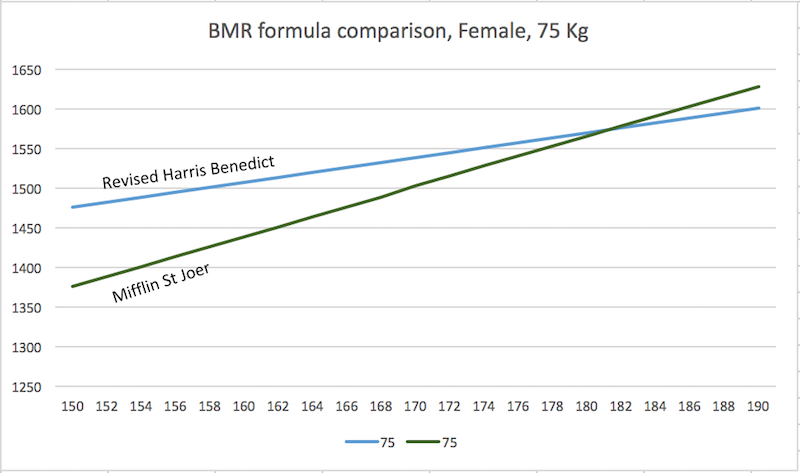
From what I've read, the Mifflin St Jeor is widely regarded to be the most accurate.
I like the one posted by @ReaderGirl3 above. http://www.sailrabbit.com/bmr/. For me it's very accurate.
it shows just the BMR...
Yeah, it's a BMR chart that @EvgeniZyntx posted saying it SHOWS as much as a 200+ variation in BMR, between the 2 formulas. It doesn't.
Sorry if I wasn't clear, across different weights and ages when you play with the equations these differences exceed 200 cals. If you'd like the worksheet, I can make it public.
Here is another study on the subject.Obes Res Clin Pract. 2015 Aug 12. pii: S1871-403X(15)00111-8. doi: 10.1016/j.orcp.2015.07.008. [Epub ahead of print]
Accuracy of resting metabolic rate prediction in overweight and obese Australian adults.
Wright TG1, Dawson B2, Jalleh G3, Guelfi KJ2.
Author information
Abstract
OBJECTIVES:
Predictive resting metabolic rate (RMR) equations in Australian populations are at least 10 years old, focused on males and do not commonly use overweight and obese weight categorisation. The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU).
METHODS:
Retrospective data from 278 participants (154 males, 124 females: 37% overweight, 63% obese) who had attended a weight management clinic were used to develop predictive RMR equations. These were then validated against another sample (from the same clinic) of 297 participants (150 males, 147 females: 47% overweight, 53% obese), and their accuracy compared with known standard equations.
RESULTS:
For the prediction sample, weight, BMI, resting VO2 and measured RMR were significantly greater in the obese than overweight. Using the validation sample, the predictive equations met a ±10% of measured RMR criterion 42% (females), 41% (total sample) and 40% (males) of the time. Prediction accuracy was not improved by using specific overweight and obese weight category equations, or by applying the known standard equations from the literature.
CONCLUSIONS:
In our sample of overweight and obese adults, RMR prediction to within ±10% of the measured value was only accurate ∼40% of the time, regardless of gender and weight classification. In clinical weight management settings direct measures of RMR should be made wherever possible.
See the bold.
"The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU)"
Looks like they developed their own NEW predictive equations and found THOSE to be only accurate 40% of the time.
Meanwhile this study -http://www.ncbi.nlm.nih.gov/pubmed/15883556 - found that:
"Four prediction equations were identified as the most commonly used in clinical practice (Harris-Benedict, Mifflin-St Jeor, Owen, and World Health Organization/Food and Agriculture Organization/United Nations University [WHO/FAO/UNU]). Of these equations, the Mifflin-St Jeor equation was the most reliable, predicting RMR within 10% of measured in more nonobese and obese individuals than any other equation, and it also had the narrowest error range."
The point is that if someone wants 100% accuracy, they can go get tested in a lab, OR they can use the most accurate formula/calculator available as a guide or starting point and see how it matches with their reality and adjust from there as most people do quite successfully.
From your article:
"For members of groups that are greatly underrepresented by existing validation studies of predictive equations, a high level of suspicion regarding the accuracy of the equations is warranted."
"Older adults and US-residing ethnic minorities were underrepresented both in the development of predictive equations and in validation studies."
And several other studies show issues with older groups or obese groups or Koreans or African-Americans or Brazilians, etc...
These are simple linear best fit equations and just do not do a good job at individual estimators if you spend some time with the research.
In the article the Miffin - St Jeor accuracy is reported to drop to 70% of the population for the obese with maximum underestimates of 20% and overestimates of 15%. That's pretty wide.
Here is a summary graph, from the study you cited.
Note that 10% accuracy means ± 200-300 error on TDEE and would still be considered accurate. For 25-30% of the population, the estimation falls outside of this accuracy.
Apologies to the OP for going off on this tangent.
Thanks for posting the chart. I only have access to the abstract so it's nice to see some details. I think for the formula to be within 10% accuracy for the vast majority (70-82%), is pretty good. And I said earlier, it's a best estimate (short of a lab test) and a point of reference. I can't imagine anyone expects it to be exact, so to me a 200-300 margin of error is not alarming. Even nutrition labels are allowed to be 10-20% off so whenever I aim for 1700 calories I'm aware it could be as much as 170-340 calories more. But like the calculators, it's the best information I have so I work with that and then use real world results to decide what changes to make.
You're welcome.
Here is the study if you want to review it yourself. https://www.andeal.org/files/Docs/Frankenfield_et_al_2005[1].pdf
I'm not sure I'd call 70% the "vast" majority.
The fact that you are aware of the variance is good, actually on the boards often people treat calorie measures (TDEE or on the package) as absolutes.
In fact, even in the field of science, people sometimes take these as rigorously correct.
Here is one example, from a pubmed search:J Am Diet Assoc. 2008 Jun;108(6):1003-8. doi: 10.1016/j.jada.2008.03.006.
Underreporting of energy intake and associated factors in a Latino population at risk of developing type 2 diabetes.
Olendzki BC1, Ma Y, Hébert JR, Pagoto SL, Merriam PA, Rosal MC, Ockene IS.
Author information
Abstract
The objective of this study was to examine the extent of underreporting of total energy intake and associated factors in a low-income, low-literacy, predominantly Caribbean Latino community in Lawrence, MA. Two hundred fifteen Latinos participated in a diabetes prevention study, for which eligibility included a >or=30% risk of developing diabetes in 7.5 years. Dietary self-reported energy intake was assessed using three randomly selected days of 24-hour diet recalls. Basal metabolic rate (BMR) was estimated using the Mifflin-St Jeor equation. Underreporting was determined by computing a ratio of energy intake to BMR, with a ratio of 1.55 expected for sedentary populations. Linear regression analyses were used to identify factors associated with underreporting (energy intake:BMR ratio). The population was predominately women (77%), middle-aged (mean 52+/-11 years), obese (78% had a body mass index >or=30); low-literate (62% < high school education), unemployed (57% reported no job), married or living with partner (52%), and some had a family history of diabetes (37% had siblings with diabetes). Reported total daily energy intake was 1,540+/-599 kcal, whereas estimated BMR was 1,495.7+/-245.1 kcal/day. When multiplied by an activity factor (1.20 for sedentariness), expected energy intake was 1,794+/-294.0 per day, indicating underreporting by an average of 254 kcal/day. Mean energy intake:BMR was 1.03+/-0.37, and was lower for participants with higher body mass index, siblings with diabetes, sedentary lifestyle, and those who were unemployed. Energy intake underreporting is prevalent in this low-income, low-literacy Caribbean Latino population. Future studies are needed to develop dietary assessment measures that minimise underreporting in this population.
The used the Mifflin-St Jeor equation in a population where it is know to be inaccurate and then when people report consumption under that estimate they then calculate that they are under reporting by that difference (see my bold) :huh:
I think this is probably worth its own thread....0 -
lemurcat12 wrote: »The differences in TDEE calculators is going to be type of calculator (basically the main ones are Katch-McArdle, which uses BF%, Mifflin-St Jeor (what MFP uses for BMR and seemingly the most common), and Harris-Benedict).
For BMR, they give me (at goal of 120, assuming BF% of 22%, which makes sense with my most recent DEXA):
M-SJ=1155
H-B=1257
K-M=1289
I think BF% is the most accurate, so assuming I felt good about that measurement's accuracy, and did not have other numbers, I'd start with that.
Then the other variable is the activity factor. One way I've seen it is 1.2 for truly sedentary, 1.375 for lightly active, 1.5 or 1.55 for moderate, 1.725 for active, and 1.9 for extremely active.
Gives a wide range (more at higher levels of activity) and much room for error, for sure, which is why using your own numbers makes sense.
My own results (based on current weight of 125, not goal) is consistent with what the calculations would suggest for me. In that that doesn't mean much, as the range is so wide, I will say that what worked for me when I started seems to work now, in terms of estimating TDEE. I find the same calculators and estimates still seem to work (although the numbers are of course different).
It seems that most calculators on internet use that classification, but I would suggest to take a look at this document:
http://www.fao.org/3/a-y5686e.pdf
(see pages 37/38)
0 -
EvgeniZyntx wrote: »CONCLUSIONS:
No single prediction equation provides accurate and precise REE estimates in all obese adults. Mifflin equations are recommended in this population, although errors exceed 10% in 25% of those assessed. There is no evidence to support the use of prediction equations in estimating TEE in obesity.
Nice link http://onlinelibrary.wiley.com/doi/10.1111/jhn.12355/abstract
I came to a similar conclusion trying to help a 300+ lb guy, as I didn't find any published data for the RMR of anyone his size. So we can't really expect a straight line to hit a target it wasn't even intended to represent.
The use of straight line equations looks pretty flawed too, a triumph of simplicity over accuracy. But maybe for another thread.
I would expect different flux to have different outcomes, one reason I dislike MFP's "net calories" concept.
3000 calories in, 1000 calories of exercise and 2000 calories in with zero exercise are the same "net calories" but quite different fluxes. We wouldn't really expect the same outcome from the two cases surely.0 -
EvgeniZyntx wrote: »CONCLUSIONS:
No single prediction equation provides accurate and precise REE estimates in all obese adults. Mifflin equations are recommended in this population, although errors exceed 10% in 25% of those assessed. There is no evidence to support the use of prediction equations in estimating TEE in obesity.
Nice link http://onlinelibrary.wiley.com/doi/10.1111/jhn.12355/abstract
I came to a similar conclusion trying to help a 300+ lb guy, as I didn't find any published data for the RMR of anyone his size. So we can't really expect a straight line to hit a target it wasn't even intended to represent.
The use of straight line equations looks pretty flawed too, a triumph of simplicity over accuracy. But maybe for another thread.
I would expect different flux to have different outcomes, one reason I dislike MFP's "net calories" concept.
3000 calories in, 1000 calories of exercise and 2000 calories in with zero exercise are the same "net calories" but quite different fluxes. We wouldn't really expect the same outcome from the two cases surely.
Yeah, we basically ignore metabolic changes, these "fluxes", etc ... for something simple and workable. Which is fine as long as one keeps in mind that they are vastly simplified estimation and require personal adjustments and reevaluations along the way.0 -
Yes, always amusing to see people quoting their TDEE to 4 sig figs.
Winding back a quarter of a century to validation work on Doubly Labelled Water http://ajpendo.physiology.org/content/261/3/E402.short we findThe doubly labeled water method tended to underestimate energy expenditure (-2.5 +/- 5.8%, not equal to 0, range -14 to +4%), with the larger underestimate observed in heavier and fatter subjects (r = -0.82 and -0.68, P less than 0.02, respectively)0 -
Gianfranco_R wrote: »lemurcat12 wrote: »The differences in TDEE calculators is going to be type of calculator (basically the main ones are Katch-McArdle, which uses BF%, Mifflin-St Jeor (what MFP uses for BMR and seemingly the most common), and Harris-Benedict).
For BMR, they give me (at goal of 120, assuming BF% of 22%, which makes sense with my most recent DEXA):
M-SJ=1155
H-B=1257
K-M=1289
I think BF% is the most accurate, so assuming I felt good about that measurement's accuracy, and did not have other numbers, I'd start with that.
Then the other variable is the activity factor. One way I've seen it is 1.2 for truly sedentary, 1.375 for lightly active, 1.5 or 1.55 for moderate, 1.725 for active, and 1.9 for extremely active.
Gives a wide range (more at higher levels of activity) and much room for error, for sure, which is why using your own numbers makes sense.
My own results (based on current weight of 125, not goal) is consistent with what the calculations would suggest for me. In that that doesn't mean much, as the range is so wide, I will say that what worked for me when I started seems to work now, in terms of estimating TDEE. I find the same calculators and estimates still seem to work (although the numbers are of course different).
It seems that most calculators on internet use that classification, but I would suggest to take a look at this document:
http://www.fao.org/3/a-y5686e.pdf
(see pages 37/38)
Okay, although a quick skim (I will read it for real when I have a bit more time) didn't seem to be drastically different (for example, it had moderate to active at 1.55-1.75, which is about the same), and I am not saying those numbers are set in stone anyway, as even the online calculators vary on this, which is what I was saying above. Do you mind summarizing what you think I should focus on?
Another issue, obviously, is that people vary on what they think is "active" or the like. Even calculators like that at IIFYM that ask about daily activity and hours pose an issue because running for an hour a day has a different effect on TDEE than doing pilates for an hour a day and also there can be big differences, of course, on how active people are outside of intentional activity and even the job (young kids, living in a city vs a place where you drive everywhere, etc.).2 -
EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »
And they explained who the underrepresented in the study were:EvgeniZyntx wrote: »Traveler120 wrote: »
I don't know where you're trying to go with this. I think the part you should have bolded was this one:EvgeniZyntx wrote: »Traveler120 wrote: »Gianfranco_R wrote: »Traveler120 wrote: »
Even from your graph, the widest point of variation is 1375 and 1475. That's only 100 calories. I don't know where you're getting 200 or more from your graph.EvgeniZyntx wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »Exercise is extremely important when in a calorie deficitbecause without it you can actually lower the rate you use calories while resting. This was proven by a U.S.government study done in 2009. Ci/co works but what good is losing the weight if you're just going to put it back on because you are no longer burning the same amount of calories at rest as you were before you lost the weight?
https://www.nia.nih.gov/newsroom/announcements/2009/05/study-shows-metabolic-adaptation-calorie-restriction
May I ask how long you've been in maintenance? 3 years into maintenance here, and I didn't exercise at all during my weight loss phase. My TDEE is spot on and has been since I started this whole thing back in 2012.
If you look at my profile it is obvious that I am not into maintenance "here." I did however lose 38 pounds about 28 years ago from diet and exercise and did a pretty good job of maintaining it until about 7 years ago. That would put me in maintenance for about 21 years. Of course that was before MFP. Exercise is important during weight loss to preserve our bone mass and metabolism as we get older. If you're happy and your TDEE is spot on then I'm happy for you. Not everyone is as lucky.
Yes, people keep telling my I'm a lucky freak of nature special snowflake TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
These formulas are very rough estimators - here is an example graph of two leading formulas. If you find them accurate it is just confirmation bias. In every study they only correspond to about 65% of metabolic factors.
For example, consider women weighing 75Kg of different heights, you'll see that the equations only match at one point and may differ as much as 200 cals (or more).
From what I've read, the Mifflin St Jeor is widely regarded to be the most accurate.
I like the one posted by @ReaderGirl3 above. http://www.sailrabbit.com/bmr/. For me it's very accurate.
it shows just the BMR...
Yeah, it's a BMR chart that @EvgeniZyntx posted saying it SHOWS as much as a 200+ variation in BMR, between the 2 formulas. It doesn't.
Sorry if I wasn't clear, across different weights and ages when you play with the equations these differences exceed 200 cals. If you'd like the worksheet, I can make it public.
Here is another study on the subject.Obes Res Clin Pract. 2015 Aug 12. pii: S1871-403X(15)00111-8. doi: 10.1016/j.orcp.2015.07.008. [Epub ahead of print]
Accuracy of resting metabolic rate prediction in overweight and obese Australian adults.
Wright TG1, Dawson B2, Jalleh G3, Guelfi KJ2.
Author information
Abstract
OBJECTIVES:
Predictive resting metabolic rate (RMR) equations in Australian populations are at least 10 years old, focused on males and do not commonly use overweight and obese weight categorisation. The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU).
METHODS:
Retrospective data from 278 participants (154 males, 124 females: 37% overweight, 63% obese) who had attended a weight management clinic were used to develop predictive RMR equations. These were then validated against another sample (from the same clinic) of 297 participants (150 males, 147 females: 47% overweight, 53% obese), and their accuracy compared with known standard equations.
RESULTS:
For the prediction sample, weight, BMI, resting VO2 and measured RMR were significantly greater in the obese than overweight. Using the validation sample, the predictive equations met a ±10% of measured RMR criterion 42% (females), 41% (total sample) and 40% (males) of the time. Prediction accuracy was not improved by using specific overweight and obese weight category equations, or by applying the known standard equations from the literature.
CONCLUSIONS:
In our sample of overweight and obese adults, RMR prediction to within ±10% of the measured value was only accurate ∼40% of the time, regardless of gender and weight classification. In clinical weight management settings direct measures of RMR should be made wherever possible.
See the bold.
"The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU)"
Looks like they developed their own NEW predictive equations and found THOSE to be only accurate 40% of the time.
Meanwhile this study -http://www.ncbi.nlm.nih.gov/pubmed/15883556 - found that:
"Four prediction equations were identified as the most commonly used in clinical practice (Harris-Benedict, Mifflin-St Jeor, Owen, and World Health Organization/Food and Agriculture Organization/United Nations University [WHO/FAO/UNU]). Of these equations, the Mifflin-St Jeor equation was the most reliable, predicting RMR within 10% of measured in more nonobese and obese individuals than any other equation, and it also had the narrowest error range."
The point is that if someone wants 100% accuracy, they can go get tested in a lab, OR they can use the most accurate formula/calculator available as a guide or starting point and see how it matches with their reality and adjust from there as most people do quite successfully.
From your article:
"For members of groups that are greatly underrepresented by existing validation studies of predictive equations, a high level of suspicion regarding the accuracy of the equations is warranted."
"Older adults and US-residing ethnic minorities were underrepresented both in the development of predictive equations and in validation studies."
And several other studies show issues with older groups or obese groups or Koreans or African-Americans or Brazilians, etc...
These are simple linear best fit equations and just do not do a good job at individual estimators if you spend some time with the research.
In the article the Miffin - St Jeor accuracy is reported to drop to 70% of the population for the obese with maximum underestimates of 20% and overestimates of 15%. That's pretty wide.
Here is a summary graph, from the study you cited.
Note that 10% accuracy means ± 200-300 error on TDEE and would still be considered accurate. For 25-30% of the population, the estimation falls outside of this accuracy.
Apologies to the OP for going off on this tangent.
Thanks for posting the chart. I only have access to the abstract so it's nice to see some details. I think for the formula to be within 10% accuracy for the vast majority (70-82%), is pretty good. And I said earlier, it's a best estimate (short of a lab test) and a point of reference. I can't imagine anyone expects it to be exact, so to me a 200-300 margin of error is not alarming. Even nutrition labels are allowed to be 10-20% off so whenever I aim for 1700 calories I'm aware it could be as much as 170-340 calories more. But like the calculators, it's the best information I have so I work with that and then use real world results to decide what changes to make.
You're welcome.
Here is the study if you want to review it yourself. https://www.andeal.org/files/Docs/Frankenfield_et_al_2005[1].pdf
I'm not sure I'd call 70% the "vast" majority.
The fact that you are aware of the variance is good, actually on the boards often people treat calorie measures (TDEE or on the package) as absolutes.
In fact, even in the field of science, people sometimes take these as rigorously correct.
Here is one example, from a pubmed search:J Am Diet Assoc. 2008 Jun;108(6):1003-8. doi: 10.1016/j.jada.2008.03.006.
Underreporting of energy intake and associated factors in a Latino population at risk of developing type 2 diabetes.
Olendzki BC1, Ma Y, Hébert JR, Pagoto SL, Merriam PA, Rosal MC, Ockene IS.
Author information
Abstract
The objective of this study was to examine the extent of underreporting of total energy intake and associated factors in a low-income, low-literacy, predominantly Caribbean Latino community in Lawrence, MA. Two hundred fifteen Latinos participated in a diabetes prevention study, for which eligibility included a >or=30% risk of developing diabetes in 7.5 years. Dietary self-reported energy intake was assessed using three randomly selected days of 24-hour diet recalls. Basal metabolic rate (BMR) was estimated using the Mifflin-St Jeor equation. Underreporting was determined by computing a ratio of energy intake to BMR, with a ratio of 1.55 expected for sedentary populations. Linear regression analyses were used to identify factors associated with underreporting (energy intake:BMR ratio). The population was predominately women (77%), middle-aged (mean 52+/-11 years), obese (78% had a body mass index >or=30); low-literate (62% < high school education), unemployed (57% reported no job), married or living with partner (52%), and some had a family history of diabetes (37% had siblings with diabetes). Reported total daily energy intake was 1,540+/-599 kcal, whereas estimated BMR was 1,495.7+/-245.1 kcal/day. When multiplied by an activity factor (1.20 for sedentariness), expected energy intake was 1,794+/-294.0 per day, indicating underreporting by an average of 254 kcal/day. Mean energy intake:BMR was 1.03+/-0.37, and was lower for participants with higher body mass index, siblings with diabetes, sedentary lifestyle, and those who were unemployed. Energy intake underreporting is prevalent in this low-income, low-literacy Caribbean Latino population. Future studies are needed to develop dietary assessment measures that minimise underreporting in this population.
The used the Mifflin-St Jeor equation in a population where it is know to be inaccurate and then when people report consumption under that estimate they then calculate that they are under reporting by that difference (see my bold) :huh:
I think this is probably worth its own thread....
What a strange study. They're trying to determine underreporting by comparing reported intake with estimated tdee? That's bizarre! Underreporting is the difference between reported intake and actual intake.
Secondly, on top of their dubious methods, they conclude that the Latino population studied is prone to underreporting, as though they're any different than any other population. Well, this study, -http://www.ncbi.nlm.nih.gov/pubmed/12396160 - used the most accurate method (the doubly labelled water method), to measure actual intake, and found that even professional dietitians were prone to underreporting as well.
"The dietitians underreported their energy intake obtained from the food records by an average of 223 +/- 116 kcal/day,.."
"Participants in the control group, as hypothesized, significantly underreported their energy intake (429 +/- 142 kcal/day, P < .05)."
(The control group comprised of non-dietitians). You'd think the dietitians, which the study said were experienced in recording intake, would be more accurate than that, especially considering they were aware that they were being studied for accuracy.
So even if we compare the 2 studies (despite different methods), the results of underreporting are virtually identical (223 cals (dieticians in this study) vs 254 cals (from your study)). I think underreporting/underestimation of intake is prevalent in general across all kinds of populations.0 -
Traveler120 wrote: »What a strange study. They're trying to determine underreporting by comparing reported intake with estimated tdee? That's bizarre! Underreporting is the difference between reported intake and actual intake.
"Actual intake" is all but unknowable, unless in a high security unit with strip searches.
But I agree that there is a long running principle in nutritional research to assume certain things are true and then use them to try to determine something else.
Examples - UK population saw increasing obesity despite declining food intake. Therefore it must be exercise. But exercise wasn't measured, and the change required isn't credible.
Doubly labelled water is used to validate intake, but DLW itself doesn't validate well against a metabolic chamber. So maybe the reported intake was spot on and it's the DLW that's at fault.0 -
Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »
And they explained who the underrepresented in the study were:EvgeniZyntx wrote: »Traveler120 wrote: »
I don't know where you're trying to go with this. I think the part you should have bolded was this one:EvgeniZyntx wrote: »Traveler120 wrote: »Gianfranco_R wrote: »Traveler120 wrote: »
Even from your graph, the widest point of variation is 1375 and 1475. That's only 100 calories. I don't know where you're getting 200 or more from your graph.EvgeniZyntx wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »Exercise is extremely important when in a calorie deficitbecause without it you can actually lower the rate you use calories while resting. This was proven by a U.S.government study done in 2009. Ci/co works but what good is losing the weight if you're just going to put it back on because you are no longer burning the same amount of calories at rest as you were before you lost the weight?
https://www.nia.nih.gov/newsroom/announcements/2009/05/study-shows-metabolic-adaptation-calorie-restriction
May I ask how long you've been in maintenance? 3 years into maintenance here, and I didn't exercise at all during my weight loss phase. My TDEE is spot on and has been since I started this whole thing back in 2012.
If you look at my profile it is obvious that I am not into maintenance "here." I did however lose 38 pounds about 28 years ago from diet and exercise and did a pretty good job of maintaining it until about 7 years ago. That would put me in maintenance for about 21 years. Of course that was before MFP. Exercise is important during weight loss to preserve our bone mass and metabolism as we get older. If you're happy and your TDEE is spot on then I'm happy for you. Not everyone is as lucky.
Yes, people keep telling my I'm a lucky freak of nature special snowflake TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
These formulas are very rough estimators - here is an example graph of two leading formulas. If you find them accurate it is just confirmation bias. In every study they only correspond to about 65% of metabolic factors.
For example, consider women weighing 75Kg of different heights, you'll see that the equations only match at one point and may differ as much as 200 cals (or more).
From what I've read, the Mifflin St Jeor is widely regarded to be the most accurate.
I like the one posted by @ReaderGirl3 above. http://www.sailrabbit.com/bmr/. For me it's very accurate.
it shows just the BMR...
Yeah, it's a BMR chart that @EvgeniZyntx posted saying it SHOWS as much as a 200+ variation in BMR, between the 2 formulas. It doesn't.
Sorry if I wasn't clear, across different weights and ages when you play with the equations these differences exceed 200 cals. If you'd like the worksheet, I can make it public.
Here is another study on the subject.Obes Res Clin Pract. 2015 Aug 12. pii: S1871-403X(15)00111-8. doi: 10.1016/j.orcp.2015.07.008. [Epub ahead of print]
Accuracy of resting metabolic rate prediction in overweight and obese Australian adults.
Wright TG1, Dawson B2, Jalleh G3, Guelfi KJ2.
Author information
Abstract
OBJECTIVES:
Predictive resting metabolic rate (RMR) equations in Australian populations are at least 10 years old, focused on males and do not commonly use overweight and obese weight categorisation. The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU).
METHODS:
Retrospective data from 278 participants (154 males, 124 females: 37% overweight, 63% obese) who had attended a weight management clinic were used to develop predictive RMR equations. These were then validated against another sample (from the same clinic) of 297 participants (150 males, 147 females: 47% overweight, 53% obese), and their accuracy compared with known standard equations.
RESULTS:
For the prediction sample, weight, BMI, resting VO2 and measured RMR were significantly greater in the obese than overweight. Using the validation sample, the predictive equations met a ±10% of measured RMR criterion 42% (females), 41% (total sample) and 40% (males) of the time. Prediction accuracy was not improved by using specific overweight and obese weight category equations, or by applying the known standard equations from the literature.
CONCLUSIONS:
In our sample of overweight and obese adults, RMR prediction to within ±10% of the measured value was only accurate ∼40% of the time, regardless of gender and weight classification. In clinical weight management settings direct measures of RMR should be made wherever possible.
See the bold.
"The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU)"
Looks like they developed their own NEW predictive equations and found THOSE to be only accurate 40% of the time.
Meanwhile this study -http://www.ncbi.nlm.nih.gov/pubmed/15883556 - found that:
"Four prediction equations were identified as the most commonly used in clinical practice (Harris-Benedict, Mifflin-St Jeor, Owen, and World Health Organization/Food and Agriculture Organization/United Nations University [WHO/FAO/UNU]). Of these equations, the Mifflin-St Jeor equation was the most reliable, predicting RMR within 10% of measured in more nonobese and obese individuals than any other equation, and it also had the narrowest error range."
The point is that if someone wants 100% accuracy, they can go get tested in a lab, OR they can use the most accurate formula/calculator available as a guide or starting point and see how it matches with their reality and adjust from there as most people do quite successfully.
From your article:
"For members of groups that are greatly underrepresented by existing validation studies of predictive equations, a high level of suspicion regarding the accuracy of the equations is warranted."
"Older adults and US-residing ethnic minorities were underrepresented both in the development of predictive equations and in validation studies."
And several other studies show issues with older groups or obese groups or Koreans or African-Americans or Brazilians, etc...
These are simple linear best fit equations and just do not do a good job at individual estimators if you spend some time with the research.
In the article the Miffin - St Jeor accuracy is reported to drop to 70% of the population for the obese with maximum underestimates of 20% and overestimates of 15%. That's pretty wide.
Here is a summary graph, from the study you cited.
Note that 10% accuracy means ± 200-300 error on TDEE and would still be considered accurate. For 25-30% of the population, the estimation falls outside of this accuracy.
Apologies to the OP for going off on this tangent.
Thanks for posting the chart. I only have access to the abstract so it's nice to see some details. I think for the formula to be within 10% accuracy for the vast majority (70-82%), is pretty good. And I said earlier, it's a best estimate (short of a lab test) and a point of reference. I can't imagine anyone expects it to be exact, so to me a 200-300 margin of error is not alarming. Even nutrition labels are allowed to be 10-20% off so whenever I aim for 1700 calories I'm aware it could be as much as 170-340 calories more. But like the calculators, it's the best information I have so I work with that and then use real world results to decide what changes to make.
You're welcome.
Here is the study if you want to review it yourself. https://www.andeal.org/files/Docs/Frankenfield_et_al_2005[1].pdf
I'm not sure I'd call 70% the "vast" majority.
The fact that you are aware of the variance is good, actually on the boards often people treat calorie measures (TDEE or on the package) as absolutes.
In fact, even in the field of science, people sometimes take these as rigorously correct.
Here is one example, from a pubmed search:J Am Diet Assoc. 2008 Jun;108(6):1003-8. doi: 10.1016/j.jada.2008.03.006.
Underreporting of energy intake and associated factors in a Latino population at risk of developing type 2 diabetes.
Olendzki BC1, Ma Y, Hébert JR, Pagoto SL, Merriam PA, Rosal MC, Ockene IS.
Author information
Abstract
The objective of this study was to examine the extent of underreporting of total energy intake and associated factors in a low-income, low-literacy, predominantly Caribbean Latino community in Lawrence, MA. Two hundred fifteen Latinos participated in a diabetes prevention study, for which eligibility included a >or=30% risk of developing diabetes in 7.5 years. Dietary self-reported energy intake was assessed using three randomly selected days of 24-hour diet recalls. Basal metabolic rate (BMR) was estimated using the Mifflin-St Jeor equation. Underreporting was determined by computing a ratio of energy intake to BMR, with a ratio of 1.55 expected for sedentary populations. Linear regression analyses were used to identify factors associated with underreporting (energy intake:BMR ratio). The population was predominately women (77%), middle-aged (mean 52+/-11 years), obese (78% had a body mass index >or=30); low-literate (62% < high school education), unemployed (57% reported no job), married or living with partner (52%), and some had a family history of diabetes (37% had siblings with diabetes). Reported total daily energy intake was 1,540+/-599 kcal, whereas estimated BMR was 1,495.7+/-245.1 kcal/day. When multiplied by an activity factor (1.20 for sedentariness), expected energy intake was 1,794+/-294.0 per day, indicating underreporting by an average of 254 kcal/day. Mean energy intake:BMR was 1.03+/-0.37, and was lower for participants with higher body mass index, siblings with diabetes, sedentary lifestyle, and those who were unemployed. Energy intake underreporting is prevalent in this low-income, low-literacy Caribbean Latino population. Future studies are needed to develop dietary assessment measures that minimise underreporting in this population.
The used the Mifflin-St Jeor equation in a population where it is know to be inaccurate and then when people report consumption under that estimate they then calculate that they are under reporting by that difference (see my bold) :huh:
I think this is probably worth its own thread....
What a strange study. They're trying to determine underreporting by comparing reported intake with estimated tdee? That's bizarre! Underreporting is the difference between reported intake and actual intake.
Secondly, on top of their dubious methods, they conclude that the Latino population studied is prone to underreporting, as though they're any different than any other population. Well, this study, -http://www.ncbi.nlm.nih.gov/pubmed/12396160 - used the most accurate method (the doubly labelled water method), to measure actual intake, and found that even professional dietitians were prone to underreporting as well.
"The dietitians underreported their energy intake obtained from the food records by an average of 223 +/- 116 kcal/day,.."
"Participants in the control group, as hypothesized, significantly underreported their energy intake (429 +/- 142 kcal/day, P < .05)."
(The control group comprised of non-dietitians). You'd think the dietitians, which the study said were experienced in recording intake, would be more accurate than that, especially considering they were aware that they were being studied for accuracy.
So even if we compare the 2 studies (despite different methods), the results of underreporting are virtually identical (223 cals (dieticians in this study) vs 254 cals (from your study)). I think underreporting/underestimation of intake is prevalent in general across all kinds of populations.
Yep, it is a very strange study. Here is the source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
What is stranger is that it is also a standard practice...
In Ireland: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
For African American Women: http://www.ncbi.nlm.nih.gov/pubmed/17197278/
It seems that using an equation that is know to overestimate can then be improperly used to report under reporting. There are literally dozens of these articles.
That's the point - that these equations, even in the sciences, are improperly uses as population predictor standards.
0 -
. duplicate .0
-
Look, we already agree on the fact that even the best tdee formulas are not 100% accurate for 100% of the general population. No disagreement there.EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »
And they explained who the underrepresented in the study were:EvgeniZyntx wrote: »Traveler120 wrote: »
I don't know where you're trying to go with this. I think the part you should have bolded was this one:EvgeniZyntx wrote: »Traveler120 wrote: »Gianfranco_R wrote: »Traveler120 wrote: »
Even from your graph, the widest point of variation is 1375 and 1475. That's only 100 calories. I don't know where you're getting 200 or more from your graph.EvgeniZyntx wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »Exercise is extremely important when in a calorie deficitbecause without it you can actually lower the rate you use calories while resting. This was proven by a U.S.government study done in 2009. Ci/co works but what good is losing the weight if you're just going to put it back on because you are no longer burning the same amount of calories at rest as you were before you lost the weight?
https://www.nia.nih.gov/newsroom/announcements/2009/05/study-shows-metabolic-adaptation-calorie-restriction
May I ask how long you've been in maintenance? 3 years into maintenance here, and I didn't exercise at all during my weight loss phase. My TDEE is spot on and has been since I started this whole thing back in 2012.
If you look at my profile it is obvious that I am not into maintenance "here." I did however lose 38 pounds about 28 years ago from diet and exercise and did a pretty good job of maintaining it until about 7 years ago. That would put me in maintenance for about 21 years. Of course that was before MFP. Exercise is important during weight loss to preserve our bone mass and metabolism as we get older. If you're happy and your TDEE is spot on then I'm happy for you. Not everyone is as lucky.
Yes, people keep telling my I'm a lucky freak of nature special snowflake TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
These formulas are very rough estimators - here is an example graph of two leading formulas. If you find them accurate it is just confirmation bias. In every study they only correspond to about 65% of metabolic factors.
For example, consider women weighing 75Kg of different heights, you'll see that the equations only match at one point and may differ as much as 200 cals (or more).
From what I've read, the Mifflin St Jeor is widely regarded to be the most accurate.
I like the one posted by @ReaderGirl3 above. http://www.sailrabbit.com/bmr/. For me it's very accurate.
it shows just the BMR...
Yeah, it's a BMR chart that @EvgeniZyntx posted saying it SHOWS as much as a 200+ variation in BMR, between the 2 formulas. It doesn't.
Sorry if I wasn't clear, across different weights and ages when you play with the equations these differences exceed 200 cals. If you'd like the worksheet, I can make it public.
Here is another study on the subject.Obes Res Clin Pract. 2015 Aug 12. pii: S1871-403X(15)00111-8. doi: 10.1016/j.orcp.2015.07.008. [Epub ahead of print]
Accuracy of resting metabolic rate prediction in overweight and obese Australian adults.
Wright TG1, Dawson B2, Jalleh G3, Guelfi KJ2.
Author information
Abstract
OBJECTIVES:
Predictive resting metabolic rate (RMR) equations in Australian populations are at least 10 years old, focused on males and do not commonly use overweight and obese weight categorisation. The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU).
METHODS:
Retrospective data from 278 participants (154 males, 124 females: 37% overweight, 63% obese) who had attended a weight management clinic were used to develop predictive RMR equations. These were then validated against another sample (from the same clinic) of 297 participants (150 males, 147 females: 47% overweight, 53% obese), and their accuracy compared with known standard equations.
RESULTS:
For the prediction sample, weight, BMI, resting VO2 and measured RMR were significantly greater in the obese than overweight. Using the validation sample, the predictive equations met a ±10% of measured RMR criterion 42% (females), 41% (total sample) and 40% (males) of the time. Prediction accuracy was not improved by using specific overweight and obese weight category equations, or by applying the known standard equations from the literature.
CONCLUSIONS:
In our sample of overweight and obese adults, RMR prediction to within ±10% of the measured value was only accurate ∼40% of the time, regardless of gender and weight classification. In clinical weight management settings direct measures of RMR should be made wherever possible.
See the bold.
"The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU)"
Looks like they developed their own NEW predictive equations and found THOSE to be only accurate 40% of the time.
Meanwhile this study -http://www.ncbi.nlm.nih.gov/pubmed/15883556 - found that:
"Four prediction equations were identified as the most commonly used in clinical practice (Harris-Benedict, Mifflin-St Jeor, Owen, and World Health Organization/Food and Agriculture Organization/United Nations University [WHO/FAO/UNU]). Of these equations, the Mifflin-St Jeor equation was the most reliable, predicting RMR within 10% of measured in more nonobese and obese individuals than any other equation, and it also had the narrowest error range."
The point is that if someone wants 100% accuracy, they can go get tested in a lab, OR they can use the most accurate formula/calculator available as a guide or starting point and see how it matches with their reality and adjust from there as most people do quite successfully.
From your article:
"For members of groups that are greatly underrepresented by existing validation studies of predictive equations, a high level of suspicion regarding the accuracy of the equations is warranted."
"Older adults and US-residing ethnic minorities were underrepresented both in the development of predictive equations and in validation studies."
And several other studies show issues with older groups or obese groups or Koreans or African-Americans or Brazilians, etc...
These are simple linear best fit equations and just do not do a good job at individual estimators if you spend some time with the research.
In the article the Miffin - St Jeor accuracy is reported to drop to 70% of the population for the obese with maximum underestimates of 20% and overestimates of 15%. That's pretty wide.
Here is a summary graph, from the study you cited.
Note that 10% accuracy means ± 200-300 error on TDEE and would still be considered accurate. For 25-30% of the population, the estimation falls outside of this accuracy.
Apologies to the OP for going off on this tangent.
Thanks for posting the chart. I only have access to the abstract so it's nice to see some details. I think for the formula to be within 10% accuracy for the vast majority (70-82%), is pretty good. And I said earlier, it's a best estimate (short of a lab test) and a point of reference. I can't imagine anyone expects it to be exact, so to me a 200-300 margin of error is not alarming. Even nutrition labels are allowed to be 10-20% off so whenever I aim for 1700 calories I'm aware it could be as much as 170-340 calories more. But like the calculators, it's the best information I have so I work with that and then use real world results to decide what changes to make.
You're welcome.
Here is the study if you want to review it yourself. https://www.andeal.org/files/Docs/Frankenfield_et_al_2005[1].pdf
I'm not sure I'd call 70% the "vast" majority.
The fact that you are aware of the variance is good, actually on the boards often people treat calorie measures (TDEE or on the package) as absolutes.
In fact, even in the field of science, people sometimes take these as rigorously correct.
Here is one example, from a pubmed search:J Am Diet Assoc. 2008 Jun;108(6):1003-8. doi: 10.1016/j.jada.2008.03.006.
Underreporting of energy intake and associated factors in a Latino population at risk of developing type 2 diabetes.
Olendzki BC1, Ma Y, Hébert JR, Pagoto SL, Merriam PA, Rosal MC, Ockene IS.
Author information
Abstract
The objective of this study was to examine the extent of underreporting of total energy intake and associated factors in a low-income, low-literacy, predominantly Caribbean Latino community in Lawrence, MA. Two hundred fifteen Latinos participated in a diabetes prevention study, for which eligibility included a >or=30% risk of developing diabetes in 7.5 years. Dietary self-reported energy intake was assessed using three randomly selected days of 24-hour diet recalls. Basal metabolic rate (BMR) was estimated using the Mifflin-St Jeor equation. Underreporting was determined by computing a ratio of energy intake to BMR, with a ratio of 1.55 expected for sedentary populations. Linear regression analyses were used to identify factors associated with underreporting (energy intake:BMR ratio). The population was predominately women (77%), middle-aged (mean 52+/-11 years), obese (78% had a body mass index >or=30); low-literate (62% < high school education), unemployed (57% reported no job), married or living with partner (52%), and some had a family history of diabetes (37% had siblings with diabetes). Reported total daily energy intake was 1,540+/-599 kcal, whereas estimated BMR was 1,495.7+/-245.1 kcal/day. When multiplied by an activity factor (1.20 for sedentariness), expected energy intake was 1,794+/-294.0 per day, indicating underreporting by an average of 254 kcal/day. Mean energy intake:BMR was 1.03+/-0.37, and was lower for participants with higher body mass index, siblings with diabetes, sedentary lifestyle, and those who were unemployed. Energy intake underreporting is prevalent in this low-income, low-literacy Caribbean Latino population. Future studies are needed to develop dietary assessment measures that minimise underreporting in this population.
The used the Mifflin-St Jeor equation in a population where it is know to be inaccurate and then when people report consumption under that estimate they then calculate that they are under reporting by that difference (see my bold) :huh:
I think this is probably worth its own thread....
What a strange study. They're trying to determine underreporting by comparing reported intake with estimated tdee? That's bizarre! Underreporting is the difference between reported intake and actual intake.
Secondly, on top of their dubious methods, they conclude that the Latino population studied is prone to underreporting, as though they're any different than any other population. Well, this study, -http://www.ncbi.nlm.nih.gov/pubmed/12396160 - used the most accurate method (the doubly labelled water method), to measure actual intake, and found that even professional dietitians were prone to underreporting as well.
"The dietitians underreported their energy intake obtained from the food records by an average of 223 +/- 116 kcal/day,.."
"Participants in the control group, as hypothesized, significantly underreported their energy intake (429 +/- 142 kcal/day, P < .05)."
(The control group comprised of non-dietitians). You'd think the dietitians, which the study said were experienced in recording intake, would be more accurate than that, especially considering they were aware that they were being studied for accuracy.
So even if we compare the 2 studies (despite different methods), the results of underreporting are virtually identical (223 cals (dieticians in this study) vs 254 cals (from your study)). I think underreporting/underestimation of intake is prevalent in general across all kinds of populations.
Yep, it is a very strange study. Here is the source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
What is stranger is that it is also a standard practice...
In Ireland: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
For African American Women: http://www.ncbi.nlm.nih.gov/pubmed/17197278/
It seems that using an equation that is know to overestimate can then be improperly used to report under reporting. There are literally dozens of these articles.
That's the point - that these equations, even in the sciences, are improperly uses as population predictor standards.
As for the issue of intake, your new study is about underreporting by black women. Your previous one was about Latinos. I don't know if I'm missing something but I think we can agree that lots of people regardless of race think they eat a lot less than they actually do, otherwise, 70% of the US wouldn't be overweight and obese.
0 -
Traveler120 wrote: »
Look, we already agree on the fact that even the best tdee formulas are not 100% accurate for 100% of the general population. No disagreement there.EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »
And they explained who the underrepresented in the study were:EvgeniZyntx wrote: »Traveler120 wrote: »
I don't know where you're trying to go with this. I think the part you should have bolded was this one:EvgeniZyntx wrote: »Traveler120 wrote: »Gianfranco_R wrote: »Traveler120 wrote: »
Even from your graph, the widest point of variation is 1375 and 1475. That's only 100 calories. I don't know where you're getting 200 or more from your graph.EvgeniZyntx wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »Exercise is extremely important when in a calorie deficitbecause without it you can actually lower the rate you use calories while resting. This was proven by a U.S.government study done in 2009. Ci/co works but what good is losing the weight if you're just going to put it back on because you are no longer burning the same amount of calories at rest as you were before you lost the weight?
https://www.nia.nih.gov/newsroom/announcements/2009/05/study-shows-metabolic-adaptation-calorie-restriction
May I ask how long you've been in maintenance? 3 years into maintenance here, and I didn't exercise at all during my weight loss phase. My TDEE is spot on and has been since I started this whole thing back in 2012.
If you look at my profile it is obvious that I am not into maintenance "here." I did however lose 38 pounds about 28 years ago from diet and exercise and did a pretty good job of maintaining it until about 7 years ago. That would put me in maintenance for about 21 years. Of course that was before MFP. Exercise is important during weight loss to preserve our bone mass and metabolism as we get older. If you're happy and your TDEE is spot on then I'm happy for you. Not everyone is as lucky.
Yes, people keep telling my I'm a lucky freak of nature special snowflake TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
These formulas are very rough estimators - here is an example graph of two leading formulas. If you find them accurate it is just confirmation bias. In every study they only correspond to about 65% of metabolic factors.
For example, consider women weighing 75Kg of different heights, you'll see that the equations only match at one point and may differ as much as 200 cals (or more).
From what I've read, the Mifflin St Jeor is widely regarded to be the most accurate.
I like the one posted by @ReaderGirl3 above. http://www.sailrabbit.com/bmr/. For me it's very accurate.
it shows just the BMR...
Yeah, it's a BMR chart that @EvgeniZyntx posted saying it SHOWS as much as a 200+ variation in BMR, between the 2 formulas. It doesn't.
Sorry if I wasn't clear, across different weights and ages when you play with the equations these differences exceed 200 cals. If you'd like the worksheet, I can make it public.
Here is another study on the subject.Obes Res Clin Pract. 2015 Aug 12. pii: S1871-403X(15)00111-8. doi: 10.1016/j.orcp.2015.07.008. [Epub ahead of print]
Accuracy of resting metabolic rate prediction in overweight and obese Australian adults.
Wright TG1, Dawson B2, Jalleh G3, Guelfi KJ2.
Author information
Abstract
OBJECTIVES:
Predictive resting metabolic rate (RMR) equations in Australian populations are at least 10 years old, focused on males and do not commonly use overweight and obese weight categorisation. The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU).
METHODS:
Retrospective data from 278 participants (154 males, 124 females: 37% overweight, 63% obese) who had attended a weight management clinic were used to develop predictive RMR equations. These were then validated against another sample (from the same clinic) of 297 participants (150 males, 147 females: 47% overweight, 53% obese), and their accuracy compared with known standard equations.
RESULTS:
For the prediction sample, weight, BMI, resting VO2 and measured RMR were significantly greater in the obese than overweight. Using the validation sample, the predictive equations met a ±10% of measured RMR criterion 42% (females), 41% (total sample) and 40% (males) of the time. Prediction accuracy was not improved by using specific overweight and obese weight category equations, or by applying the known standard equations from the literature.
CONCLUSIONS:
In our sample of overweight and obese adults, RMR prediction to within ±10% of the measured value was only accurate ∼40% of the time, regardless of gender and weight classification. In clinical weight management settings direct measures of RMR should be made wherever possible.
See the bold.
"The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU)"
Looks like they developed their own NEW predictive equations and found THOSE to be only accurate 40% of the time.
Meanwhile this study -http://www.ncbi.nlm.nih.gov/pubmed/15883556 - found that:
"Four prediction equations were identified as the most commonly used in clinical practice (Harris-Benedict, Mifflin-St Jeor, Owen, and World Health Organization/Food and Agriculture Organization/United Nations University [WHO/FAO/UNU]). Of these equations, the Mifflin-St Jeor equation was the most reliable, predicting RMR within 10% of measured in more nonobese and obese individuals than any other equation, and it also had the narrowest error range."
The point is that if someone wants 100% accuracy, they can go get tested in a lab, OR they can use the most accurate formula/calculator available as a guide or starting point and see how it matches with their reality and adjust from there as most people do quite successfully.
From your article:
"For members of groups that are greatly underrepresented by existing validation studies of predictive equations, a high level of suspicion regarding the accuracy of the equations is warranted."
"Older adults and US-residing ethnic minorities were underrepresented both in the development of predictive equations and in validation studies."
And several other studies show issues with older groups or obese groups or Koreans or African-Americans or Brazilians, etc...
These are simple linear best fit equations and just do not do a good job at individual estimators if you spend some time with the research.
In the article the Miffin - St Jeor accuracy is reported to drop to 70% of the population for the obese with maximum underestimates of 20% and overestimates of 15%. That's pretty wide.
Here is a summary graph, from the study you cited.
Note that 10% accuracy means ± 200-300 error on TDEE and would still be considered accurate. For 25-30% of the population, the estimation falls outside of this accuracy.
Apologies to the OP for going off on this tangent.
Thanks for posting the chart. I only have access to the abstract so it's nice to see some details. I think for the formula to be within 10% accuracy for the vast majority (70-82%), is pretty good. And I said earlier, it's a best estimate (short of a lab test) and a point of reference. I can't imagine anyone expects it to be exact, so to me a 200-300 margin of error is not alarming. Even nutrition labels are allowed to be 10-20% off so whenever I aim for 1700 calories I'm aware it could be as much as 170-340 calories more. But like the calculators, it's the best information I have so I work with that and then use real world results to decide what changes to make.
You're welcome.
Here is the study if you want to review it yourself. https://www.andeal.org/files/Docs/Frankenfield_et_al_2005[1].pdf
I'm not sure I'd call 70% the "vast" majority.
The fact that you are aware of the variance is good, actually on the boards often people treat calorie measures (TDEE or on the package) as absolutes.
In fact, even in the field of science, people sometimes take these as rigorously correct.
Here is one example, from a pubmed search:J Am Diet Assoc. 2008 Jun;108(6):1003-8. doi: 10.1016/j.jada.2008.03.006.
Underreporting of energy intake and associated factors in a Latino population at risk of developing type 2 diabetes.
Olendzki BC1, Ma Y, Hébert JR, Pagoto SL, Merriam PA, Rosal MC, Ockene IS.
Author information
Abstract
The objective of this study was to examine the extent of underreporting of total energy intake and associated factors in a low-income, low-literacy, predominantly Caribbean Latino community in Lawrence, MA. Two hundred fifteen Latinos participated in a diabetes prevention study, for which eligibility included a >or=30% risk of developing diabetes in 7.5 years. Dietary self-reported energy intake was assessed using three randomly selected days of 24-hour diet recalls. Basal metabolic rate (BMR) was estimated using the Mifflin-St Jeor equation. Underreporting was determined by computing a ratio of energy intake to BMR, with a ratio of 1.55 expected for sedentary populations. Linear regression analyses were used to identify factors associated with underreporting (energy intake:BMR ratio). The population was predominately women (77%), middle-aged (mean 52+/-11 years), obese (78% had a body mass index >or=30); low-literate (62% < high school education), unemployed (57% reported no job), married or living with partner (52%), and some had a family history of diabetes (37% had siblings with diabetes). Reported total daily energy intake was 1,540+/-599 kcal, whereas estimated BMR was 1,495.7+/-245.1 kcal/day. When multiplied by an activity factor (1.20 for sedentariness), expected energy intake was 1,794+/-294.0 per day, indicating underreporting by an average of 254 kcal/day. Mean energy intake:BMR was 1.03+/-0.37, and was lower for participants with higher body mass index, siblings with diabetes, sedentary lifestyle, and those who were unemployed. Energy intake underreporting is prevalent in this low-income, low-literacy Caribbean Latino population. Future studies are needed to develop dietary assessment measures that minimise underreporting in this population.
The used the Mifflin-St Jeor equation in a population where it is know to be inaccurate and then when people report consumption under that estimate they then calculate that they are under reporting by that difference (see my bold) :huh:
I think this is probably worth its own thread....
What a strange study. They're trying to determine underreporting by comparing reported intake with estimated tdee? That's bizarre! Underreporting is the difference between reported intake and actual intake.
Secondly, on top of their dubious methods, they conclude that the Latino population studied is prone to underreporting, as though they're any different than any other population. Well, this study, -http://www.ncbi.nlm.nih.gov/pubmed/12396160 - used the most accurate method (the doubly labelled water method), to measure actual intake, and found that even professional dietitians were prone to underreporting as well.
"The dietitians underreported their energy intake obtained from the food records by an average of 223 +/- 116 kcal/day,.."
"Participants in the control group, as hypothesized, significantly underreported their energy intake (429 +/- 142 kcal/day, P < .05)."
(The control group comprised of non-dietitians). You'd think the dietitians, which the study said were experienced in recording intake, would be more accurate than that, especially considering they were aware that they were being studied for accuracy.
So even if we compare the 2 studies (despite different methods), the results of underreporting are virtually identical (223 cals (dieticians in this study) vs 254 cals (from your study)). I think underreporting/underestimation of intake is prevalent in general across all kinds of populations.
Yep, it is a very strange study. Here is the source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
What is stranger is that it is also a standard practice...
In Ireland: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
For African American Women: http://www.ncbi.nlm.nih.gov/pubmed/17197278/
It seems that using an equation that is know to overestimate can then be improperly used to report under reporting. There are literally dozens of these articles.
That's the point - that these equations, even in the sciences, are improperly uses as population predictor standards.
As for the issue of intake, your new study is about underreporting by black women. Your previous one was about Latinos. I don't know if I'm missing something but I think we can agree that lots of people regardless of race think they eat a lot less than they actually do, otherwise, 70% of the US wouldn't be overweight and obese.
These studies have nothing to do with what people think they eat. They could be reporting accurately and be overeating. Or undereating and still under reporting. Studies on reporting of exercise also show under-reporting of activity. People just forget what they had or did 2-3 days ago. Some of these studies do 7 day reporting. People don't note everything or aren't particularly trained or focused to accurately complete the task.
The issue is that eat of these studies fails to consider that the equation they use as the gold standard is wrong for the populations they are studying. All 3 studies can be criticised for that part of their results.
The fact that 70% of the population is overweight isn't related to diary reporting. Improvements in diary reporting, in research testing that, don't show an improvement in weight.
3 -
Weight training has been proven to burn more calories for a longer period than cardio, just wanna throw that in there0
-
robs_ready wrote: »Weight training has been proven to burn more calories for a longer period than cardio, just wanna throw that in there
No robs, it hasn't. i assume you are talking about EPOC.
LISS running is about 7% HIIT is about 14% EPOC
Let's look at an example:
An 80 kg individual does a 60 min endurance workout and burns 640 calories. Add 45 calories for the 7% EPOC for a total of 685.
Same person does a 20 min HIIT workout and burns about 300 calories. Even with the extra EPOC of 13%, that's only an extra 40 calories, for a total of 340.
Same person does resistance training for an hour burns 300 cals and sees an EPOC increase of 10% over 24hrs (so about 180 cals for a BMR of 1800).
So
- running: 685
- HIIT: 340
- resistance training 480
take a look at http://www.bodyrecomposition.com/research-review/research-review-effects-of-exercise-intensity-and-duration-on-the-excess-post-exercise-oxygen-consumption.html/1 -
EvgeniZyntx wrote: »Traveler120 wrote: »
Look, we already agree on the fact that even the best tdee formulas are not 100% accurate for 100% of the general population. No disagreement there.EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »
And they explained who the underrepresented in the study were:EvgeniZyntx wrote: »Traveler120 wrote: »
I don't know where you're trying to go with this. I think the part you should have bolded was this one:EvgeniZyntx wrote: »Traveler120 wrote: »Gianfranco_R wrote: »Traveler120 wrote: »
Even from your graph, the widest point of variation is 1375 and 1475. That's only 100 calories. I don't know where you're getting 200 or more from your graph.EvgeniZyntx wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »Exercise is extremely important when in a calorie deficitbecause without it you can actually lower the rate you use calories while resting. This was proven by a U.S.government study done in 2009. Ci/co works but what good is losing the weight if you're just going to put it back on because you are no longer burning the same amount of calories at rest as you were before you lost the weight?
https://www.nia.nih.gov/newsroom/announcements/2009/05/study-shows-metabolic-adaptation-calorie-restriction
May I ask how long you've been in maintenance? 3 years into maintenance here, and I didn't exercise at all during my weight loss phase. My TDEE is spot on and has been since I started this whole thing back in 2012.
If you look at my profile it is obvious that I am not into maintenance "here." I did however lose 38 pounds about 28 years ago from diet and exercise and did a pretty good job of maintaining it until about 7 years ago. That would put me in maintenance for about 21 years. Of course that was before MFP. Exercise is important during weight loss to preserve our bone mass and metabolism as we get older. If you're happy and your TDEE is spot on then I'm happy for you. Not everyone is as lucky.
Yes, people keep telling my I'm a lucky freak of nature special snowflake TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
These formulas are very rough estimators - here is an example graph of two leading formulas. If you find them accurate it is just confirmation bias. In every study they only correspond to about 65% of metabolic factors.
For example, consider women weighing 75Kg of different heights, you'll see that the equations only match at one point and may differ as much as 200 cals (or more).
From what I've read, the Mifflin St Jeor is widely regarded to be the most accurate.
I like the one posted by @ReaderGirl3 above. http://www.sailrabbit.com/bmr/. For me it's very accurate.
it shows just the BMR...
Yeah, it's a BMR chart that @EvgeniZyntx posted saying it SHOWS as much as a 200+ variation in BMR, between the 2 formulas. It doesn't.
Sorry if I wasn't clear, across different weights and ages when you play with the equations these differences exceed 200 cals. If you'd like the worksheet, I can make it public.
Here is another study on the subject.Obes Res Clin Pract. 2015 Aug 12. pii: S1871-403X(15)00111-8. doi: 10.1016/j.orcp.2015.07.008. [Epub ahead of print]
Accuracy of resting metabolic rate prediction in overweight and obese Australian adults.
Wright TG1, Dawson B2, Jalleh G3, Guelfi KJ2.
Author information
Abstract
OBJECTIVES:
Predictive resting metabolic rate (RMR) equations in Australian populations are at least 10 years old, focused on males and do not commonly use overweight and obese weight categorisation. The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU).
METHODS:
Retrospective data from 278 participants (154 males, 124 females: 37% overweight, 63% obese) who had attended a weight management clinic were used to develop predictive RMR equations. These were then validated against another sample (from the same clinic) of 297 participants (150 males, 147 females: 47% overweight, 53% obese), and their accuracy compared with known standard equations.
RESULTS:
For the prediction sample, weight, BMI, resting VO2 and measured RMR were significantly greater in the obese than overweight. Using the validation sample, the predictive equations met a ±10% of measured RMR criterion 42% (females), 41% (total sample) and 40% (males) of the time. Prediction accuracy was not improved by using specific overweight and obese weight category equations, or by applying the known standard equations from the literature.
CONCLUSIONS:
In our sample of overweight and obese adults, RMR prediction to within ±10% of the measured value was only accurate ∼40% of the time, regardless of gender and weight classification. In clinical weight management settings direct measures of RMR should be made wherever possible.
See the bold.
"The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU)"
Looks like they developed their own NEW predictive equations and found THOSE to be only accurate 40% of the time.
Meanwhile this study -http://www.ncbi.nlm.nih.gov/pubmed/15883556 - found that:
"Four prediction equations were identified as the most commonly used in clinical practice (Harris-Benedict, Mifflin-St Jeor, Owen, and World Health Organization/Food and Agriculture Organization/United Nations University [WHO/FAO/UNU]). Of these equations, the Mifflin-St Jeor equation was the most reliable, predicting RMR within 10% of measured in more nonobese and obese individuals than any other equation, and it also had the narrowest error range."
The point is that if someone wants 100% accuracy, they can go get tested in a lab, OR they can use the most accurate formula/calculator available as a guide or starting point and see how it matches with their reality and adjust from there as most people do quite successfully.
From your article:
"For members of groups that are greatly underrepresented by existing validation studies of predictive equations, a high level of suspicion regarding the accuracy of the equations is warranted."
"Older adults and US-residing ethnic minorities were underrepresented both in the development of predictive equations and in validation studies."
And several other studies show issues with older groups or obese groups or Koreans or African-Americans or Brazilians, etc...
These are simple linear best fit equations and just do not do a good job at individual estimators if you spend some time with the research.
In the article the Miffin - St Jeor accuracy is reported to drop to 70% of the population for the obese with maximum underestimates of 20% and overestimates of 15%. That's pretty wide.
Here is a summary graph, from the study you cited.
Note that 10% accuracy means ± 200-300 error on TDEE and would still be considered accurate. For 25-30% of the population, the estimation falls outside of this accuracy.
Apologies to the OP for going off on this tangent.
Thanks for posting the chart. I only have access to the abstract so it's nice to see some details. I think for the formula to be within 10% accuracy for the vast majority (70-82%), is pretty good. And I said earlier, it's a best estimate (short of a lab test) and a point of reference. I can't imagine anyone expects it to be exact, so to me a 200-300 margin of error is not alarming. Even nutrition labels are allowed to be 10-20% off so whenever I aim for 1700 calories I'm aware it could be as much as 170-340 calories more. But like the calculators, it's the best information I have so I work with that and then use real world results to decide what changes to make.
You're welcome.
Here is the study if you want to review it yourself. https://www.andeal.org/files/Docs/Frankenfield_et_al_2005[1].pdf
I'm not sure I'd call 70% the "vast" majority.
The fact that you are aware of the variance is good, actually on the boards often people treat calorie measures (TDEE or on the package) as absolutes.
In fact, even in the field of science, people sometimes take these as rigorously correct.
Here is one example, from a pubmed search:J Am Diet Assoc. 2008 Jun;108(6):1003-8. doi: 10.1016/j.jada.2008.03.006.
Underreporting of energy intake and associated factors in a Latino population at risk of developing type 2 diabetes.
Olendzki BC1, Ma Y, Hébert JR, Pagoto SL, Merriam PA, Rosal MC, Ockene IS.
Author information
Abstract
The objective of this study was to examine the extent of underreporting of total energy intake and associated factors in a low-income, low-literacy, predominantly Caribbean Latino community in Lawrence, MA. Two hundred fifteen Latinos participated in a diabetes prevention study, for which eligibility included a >or=30% risk of developing diabetes in 7.5 years. Dietary self-reported energy intake was assessed using three randomly selected days of 24-hour diet recalls. Basal metabolic rate (BMR) was estimated using the Mifflin-St Jeor equation. Underreporting was determined by computing a ratio of energy intake to BMR, with a ratio of 1.55 expected for sedentary populations. Linear regression analyses were used to identify factors associated with underreporting (energy intake:BMR ratio). The population was predominately women (77%), middle-aged (mean 52+/-11 years), obese (78% had a body mass index >or=30); low-literate (62% < high school education), unemployed (57% reported no job), married or living with partner (52%), and some had a family history of diabetes (37% had siblings with diabetes). Reported total daily energy intake was 1,540+/-599 kcal, whereas estimated BMR was 1,495.7+/-245.1 kcal/day. When multiplied by an activity factor (1.20 for sedentariness), expected energy intake was 1,794+/-294.0 per day, indicating underreporting by an average of 254 kcal/day. Mean energy intake:BMR was 1.03+/-0.37, and was lower for participants with higher body mass index, siblings with diabetes, sedentary lifestyle, and those who were unemployed. Energy intake underreporting is prevalent in this low-income, low-literacy Caribbean Latino population. Future studies are needed to develop dietary assessment measures that minimise underreporting in this population.
The used the Mifflin-St Jeor equation in a population where it is know to be inaccurate and then when people report consumption under that estimate they then calculate that they are under reporting by that difference (see my bold) :huh:
I think this is probably worth its own thread....
What a strange study. They're trying to determine underreporting by comparing reported intake with estimated tdee? That's bizarre! Underreporting is the difference between reported intake and actual intake.
Secondly, on top of their dubious methods, they conclude that the Latino population studied is prone to underreporting, as though they're any different than any other population. Well, this study, -http://www.ncbi.nlm.nih.gov/pubmed/12396160 - used the most accurate method (the doubly labelled water method), to measure actual intake, and found that even professional dietitians were prone to underreporting as well.
"The dietitians underreported their energy intake obtained from the food records by an average of 223 +/- 116 kcal/day,.."
"Participants in the control group, as hypothesized, significantly underreported their energy intake (429 +/- 142 kcal/day, P < .05)."
(The control group comprised of non-dietitians). You'd think the dietitians, which the study said were experienced in recording intake, would be more accurate than that, especially considering they were aware that they were being studied for accuracy.
So even if we compare the 2 studies (despite different methods), the results of underreporting are virtually identical (223 cals (dieticians in this study) vs 254 cals (from your study)). I think underreporting/underestimation of intake is prevalent in general across all kinds of populations.
Yep, it is a very strange study. Here is the source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
What is stranger is that it is also a standard practice...
In Ireland: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
For African American Women: http://www.ncbi.nlm.nih.gov/pubmed/17197278/
It seems that using an equation that is know to overestimate can then be improperly used to report under reporting. There are literally dozens of these articles.
That's the point - that these equations, even in the sciences, are improperly uses as population predictor standards.
As for the issue of intake, your new study is about underreporting by black women. Your previous one was about Latinos. I don't know if I'm missing something but I think we can agree that lots of people regardless of race think they eat a lot less than they actually do, otherwise, 70% of the US wouldn't be overweight and obese.
These studies have nothing to do with what people think they eat. They could be reporting accurately and be overeating. Or undereating and still under reporting. Studies on reporting of exercise also show under-reporting of activity. People just forget what they had or did 2-3 days ago. Some of these studies do 7 day reporting. People don't note everything or aren't particularly trained or focused to accurately complete the task.
The issue is that eat of these studies fails to consider that the equation they use as the gold standard is wrong for the populations they are studying. All 3 studies can be criticised for that part of their results.
The fact that 70% of the population is overweight isn't related to diary reporting. Improvements in diary reporting, in research testing that, don't show an improvement in weight.
Ah ok, my bad. I mistakenly thought that 70% are overweight not because of inaccurate tdee equations, but because they eat too much (and underestimate intake) and exercise too little (and overestimate tdee). I stand corrected.0 -
Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »
Look, we already agree on the fact that even the best tdee formulas are not 100% accurate for 100% of the general population. No disagreement there.EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »EvgeniZyntx wrote: »Traveler120 wrote: »
And they explained who the underrepresented in the study were:EvgeniZyntx wrote: »Traveler120 wrote: »
I don't know where you're trying to go with this. I think the part you should have bolded was this one:EvgeniZyntx wrote: »Traveler120 wrote: »Gianfranco_R wrote: »Traveler120 wrote: »
Even from your graph, the widest point of variation is 1375 and 1475. That's only 100 calories. I don't know where you're getting 200 or more from your graph.EvgeniZyntx wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »Exercise is extremely important when in a calorie deficitbecause without it you can actually lower the rate you use calories while resting. This was proven by a U.S.government study done in 2009. Ci/co works but what good is losing the weight if you're just going to put it back on because you are no longer burning the same amount of calories at rest as you were before you lost the weight?
https://www.nia.nih.gov/newsroom/announcements/2009/05/study-shows-metabolic-adaptation-calorie-restriction
May I ask how long you've been in maintenance? 3 years into maintenance here, and I didn't exercise at all during my weight loss phase. My TDEE is spot on and has been since I started this whole thing back in 2012.
If you look at my profile it is obvious that I am not into maintenance "here." I did however lose 38 pounds about 28 years ago from diet and exercise and did a pretty good job of maintaining it until about 7 years ago. That would put me in maintenance for about 21 years. Of course that was before MFP. Exercise is important during weight loss to preserve our bone mass and metabolism as we get older. If you're happy and your TDEE is spot on then I'm happy for you. Not everyone is as lucky.
Yes, people keep telling my I'm a lucky freak of nature special snowflake TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
These formulas are very rough estimators - here is an example graph of two leading formulas. If you find them accurate it is just confirmation bias. In every study they only correspond to about 65% of metabolic factors.
For example, consider women weighing 75Kg of different heights, you'll see that the equations only match at one point and may differ as much as 200 cals (or more).
From what I've read, the Mifflin St Jeor is widely regarded to be the most accurate.
I like the one posted by @ReaderGirl3 above. http://www.sailrabbit.com/bmr/. For me it's very accurate.
it shows just the BMR...
Yeah, it's a BMR chart that @EvgeniZyntx posted saying it SHOWS as much as a 200+ variation in BMR, between the 2 formulas. It doesn't.
Sorry if I wasn't clear, across different weights and ages when you play with the equations these differences exceed 200 cals. If you'd like the worksheet, I can make it public.
Here is another study on the subject.Obes Res Clin Pract. 2015 Aug 12. pii: S1871-403X(15)00111-8. doi: 10.1016/j.orcp.2015.07.008. [Epub ahead of print]
Accuracy of resting metabolic rate prediction in overweight and obese Australian adults.
Wright TG1, Dawson B2, Jalleh G3, Guelfi KJ2.
Author information
Abstract
OBJECTIVES:
Predictive resting metabolic rate (RMR) equations in Australian populations are at least 10 years old, focused on males and do not commonly use overweight and obese weight categorisation. The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU).
METHODS:
Retrospective data from 278 participants (154 males, 124 females: 37% overweight, 63% obese) who had attended a weight management clinic were used to develop predictive RMR equations. These were then validated against another sample (from the same clinic) of 297 participants (150 males, 147 females: 47% overweight, 53% obese), and their accuracy compared with known standard equations.
RESULTS:
For the prediction sample, weight, BMI, resting VO2 and measured RMR were significantly greater in the obese than overweight. Using the validation sample, the predictive equations met a ±10% of measured RMR criterion 42% (females), 41% (total sample) and 40% (males) of the time. Prediction accuracy was not improved by using specific overweight and obese weight category equations, or by applying the known standard equations from the literature.
CONCLUSIONS:
In our sample of overweight and obese adults, RMR prediction to within ±10% of the measured value was only accurate ∼40% of the time, regardless of gender and weight classification. In clinical weight management settings direct measures of RMR should be made wherever possible.
See the bold.
"The aim of this study was to measure RMR via indirect calorimetry in overweight and obese Australian adults to develop population specific predictive equations and compare with other well-known international equations (Mifflin-St. Jeor, Owen and WHO/FAO/UNU)"
Looks like they developed their own NEW predictive equations and found THOSE to be only accurate 40% of the time.
Meanwhile this study -http://www.ncbi.nlm.nih.gov/pubmed/15883556 - found that:
"Four prediction equations were identified as the most commonly used in clinical practice (Harris-Benedict, Mifflin-St Jeor, Owen, and World Health Organization/Food and Agriculture Organization/United Nations University [WHO/FAO/UNU]). Of these equations, the Mifflin-St Jeor equation was the most reliable, predicting RMR within 10% of measured in more nonobese and obese individuals than any other equation, and it also had the narrowest error range."
The point is that if someone wants 100% accuracy, they can go get tested in a lab, OR they can use the most accurate formula/calculator available as a guide or starting point and see how it matches with their reality and adjust from there as most people do quite successfully.
From your article:
"For members of groups that are greatly underrepresented by existing validation studies of predictive equations, a high level of suspicion regarding the accuracy of the equations is warranted."
"Older adults and US-residing ethnic minorities were underrepresented both in the development of predictive equations and in validation studies."
And several other studies show issues with older groups or obese groups or Koreans or African-Americans or Brazilians, etc...
These are simple linear best fit equations and just do not do a good job at individual estimators if you spend some time with the research.
In the article the Miffin - St Jeor accuracy is reported to drop to 70% of the population for the obese with maximum underestimates of 20% and overestimates of 15%. That's pretty wide.
Here is a summary graph, from the study you cited.
Note that 10% accuracy means ± 200-300 error on TDEE and would still be considered accurate. For 25-30% of the population, the estimation falls outside of this accuracy.
Apologies to the OP for going off on this tangent.
Thanks for posting the chart. I only have access to the abstract so it's nice to see some details. I think for the formula to be within 10% accuracy for the vast majority (70-82%), is pretty good. And I said earlier, it's a best estimate (short of a lab test) and a point of reference. I can't imagine anyone expects it to be exact, so to me a 200-300 margin of error is not alarming. Even nutrition labels are allowed to be 10-20% off so whenever I aim for 1700 calories I'm aware it could be as much as 170-340 calories more. But like the calculators, it's the best information I have so I work with that and then use real world results to decide what changes to make.
You're welcome.
Here is the study if you want to review it yourself. https://www.andeal.org/files/Docs/Frankenfield_et_al_2005[1].pdf
I'm not sure I'd call 70% the "vast" majority.
The fact that you are aware of the variance is good, actually on the boards often people treat calorie measures (TDEE or on the package) as absolutes.
In fact, even in the field of science, people sometimes take these as rigorously correct.
Here is one example, from a pubmed search:J Am Diet Assoc. 2008 Jun;108(6):1003-8. doi: 10.1016/j.jada.2008.03.006.
Underreporting of energy intake and associated factors in a Latino population at risk of developing type 2 diabetes.
Olendzki BC1, Ma Y, Hébert JR, Pagoto SL, Merriam PA, Rosal MC, Ockene IS.
Author information
Abstract
The objective of this study was to examine the extent of underreporting of total energy intake and associated factors in a low-income, low-literacy, predominantly Caribbean Latino community in Lawrence, MA. Two hundred fifteen Latinos participated in a diabetes prevention study, for which eligibility included a >or=30% risk of developing diabetes in 7.5 years. Dietary self-reported energy intake was assessed using three randomly selected days of 24-hour diet recalls. Basal metabolic rate (BMR) was estimated using the Mifflin-St Jeor equation. Underreporting was determined by computing a ratio of energy intake to BMR, with a ratio of 1.55 expected for sedentary populations. Linear regression analyses were used to identify factors associated with underreporting (energy intake:BMR ratio). The population was predominately women (77%), middle-aged (mean 52+/-11 years), obese (78% had a body mass index >or=30); low-literate (62% < high school education), unemployed (57% reported no job), married or living with partner (52%), and some had a family history of diabetes (37% had siblings with diabetes). Reported total daily energy intake was 1,540+/-599 kcal, whereas estimated BMR was 1,495.7+/-245.1 kcal/day. When multiplied by an activity factor (1.20 for sedentariness), expected energy intake was 1,794+/-294.0 per day, indicating underreporting by an average of 254 kcal/day. Mean energy intake:BMR was 1.03+/-0.37, and was lower for participants with higher body mass index, siblings with diabetes, sedentary lifestyle, and those who were unemployed. Energy intake underreporting is prevalent in this low-income, low-literacy Caribbean Latino population. Future studies are needed to develop dietary assessment measures that minimise underreporting in this population.
The used the Mifflin-St Jeor equation in a population where it is know to be inaccurate and then when people report consumption under that estimate they then calculate that they are under reporting by that difference (see my bold) :huh:
I think this is probably worth its own thread....
What a strange study. They're trying to determine underreporting by comparing reported intake with estimated tdee? That's bizarre! Underreporting is the difference between reported intake and actual intake.
Secondly, on top of their dubious methods, they conclude that the Latino population studied is prone to underreporting, as though they're any different than any other population. Well, this study, -http://www.ncbi.nlm.nih.gov/pubmed/12396160 - used the most accurate method (the doubly labelled water method), to measure actual intake, and found that even professional dietitians were prone to underreporting as well.
"The dietitians underreported their energy intake obtained from the food records by an average of 223 +/- 116 kcal/day,.."
"Participants in the control group, as hypothesized, significantly underreported their energy intake (429 +/- 142 kcal/day, P < .05)."
(The control group comprised of non-dietitians). You'd think the dietitians, which the study said were experienced in recording intake, would be more accurate than that, especially considering they were aware that they were being studied for accuracy.
So even if we compare the 2 studies (despite different methods), the results of underreporting are virtually identical (223 cals (dieticians in this study) vs 254 cals (from your study)). I think underreporting/underestimation of intake is prevalent in general across all kinds of populations.
Yep, it is a very strange study. Here is the source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
What is stranger is that it is also a standard practice...
In Ireland: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4017735/
For African American Women: http://www.ncbi.nlm.nih.gov/pubmed/17197278/
It seems that using an equation that is know to overestimate can then be improperly used to report under reporting. There are literally dozens of these articles.
That's the point - that these equations, even in the sciences, are improperly uses as population predictor standards.
As for the issue of intake, your new study is about underreporting by black women. Your previous one was about Latinos. I don't know if I'm missing something but I think we can agree that lots of people regardless of race think they eat a lot less than they actually do, otherwise, 70% of the US wouldn't be overweight and obese.
These studies have nothing to do with what people think they eat. They could be reporting accurately and be overeating. Or undereating and still under reporting. Studies on reporting of exercise also show under-reporting of activity. People just forget what they had or did 2-3 days ago. Some of these studies do 7 day reporting. People don't note everything or aren't particularly trained or focused to accurately complete the task.
The issue is that eat of these studies fails to consider that the equation they use as the gold standard is wrong for the populations they are studying. All 3 studies can be criticised for that part of their results.
The fact that 70% of the population is overweight isn't related to diary reporting. Improvements in diary reporting, in research testing that, don't show an improvement in weight.
Ah ok, my bad. I mistakenly thought that 70% are overweight not because of inaccurate tdee equations, but because they eat too much (and underestimate intake) and exercise too little (and overestimate tdee). I stand corrected.
:huh: I got nothing.
0 -
Traveler120 wrote: »Ah ok, my bad. I mistakenly thought that 70% are overweight not because of inaccurate tdee equations, but because they eat too much (and underestimate intake) and exercise too little (and overestimate tdee). I stand corrected.
He wasn't saying that people gained weight due to inaccurate TDEE (or anything about how people gain weight). At least, that wasn't my interpretation. He was showing how TDEE estimates from the calculators may be misused, even in scientific studies--here to indicate underreporting by various groups of people. That in some of these cases the groups are those for whom the typical estimated TDEEs from the calculators have been shown to be less accurate on average makes this especially problematic (although assuming that estimated TDEE=real TDEE would be a problem in any case).0 -
Gianfranco_R wrote: »lemurcat12 wrote: »The differences in TDEE calculators is going to be type of calculator (basically the main ones are Katch-McArdle, which uses BF%, Mifflin-St Jeor (what MFP uses for BMR and seemingly the most common), and Harris-Benedict).
For BMR, they give me (at goal of 120, assuming BF% of 22%, which makes sense with my most recent DEXA):
M-SJ=1155
H-B=1257
K-M=1289
I think BF% is the most accurate, so assuming I felt good about that measurement's accuracy, and did not have other numbers, I'd start with that.
Then the other variable is the activity factor. One way I've seen it is 1.2 for truly sedentary, 1.375 for lightly active, 1.5 or 1.55 for moderate, 1.725 for active, and 1.9 for extremely active.
Gives a wide range (more at higher levels of activity) and much room for error, for sure, which is why using your own numbers makes sense.
My own results (based on current weight of 125, not goal) is consistent with what the calculations would suggest for me. In that that doesn't mean much, as the range is so wide, I will say that what worked for me when I started seems to work now, in terms of estimating TDEE. I find the same calculators and estimates still seem to work (although the numbers are of course different).
It seems that most calculators on internet use that classification, but I would suggest to take a look at this document:
http://www.fao.org/3/a-y5686e.pdf
(see pages 37/38)
Okay, I have. Significantly higher. I wonder if that's because the numbers I quoted are more US-focused. The FAO report mentioned, for sedentary, someone living in a city with a sedentary job or a woman in African with a home-based business -- both likely to be more active than someone in the US who genuinely can drive everywhere in addition to having a sedentary job and may have lots of conveniences at home. I did find that even when I started and thought I was sedentary that my numbers were more like lightly active, which I attributed to living in a quite walkable big city and rarely driving. I'd think that's more like many Europeans (but who knows, I'm American so could be working on stereotypes).
I certainly would agree that the multiplier used and figuring out what it should be is a huge subjective factor. Lots of people think they are sedentary but aren't, and others probably think they are more active and aren't.
Thoughts?0 -
At the very least, exercising more, and eating more, gives you more opportunities to eat a variety of foods and get more nutrients.0
-
lemurcat12 wrote: »Traveler120 wrote: »Ah ok, my bad. I mistakenly thought that 70% are overweight not because of inaccurate tdee equations, but because they eat too much (and underestimate intake) and exercise too little (and overestimate tdee). I stand corrected.
He wasn't saying that people gained weight due to inaccurate TDEE (or anything about how people gain weight). At least, that wasn't my interpretation. He was showing how TDEE estimates from the calculators may be misused, even in scientific studies--here to indicate underreporting by various groups of people. That in some of these cases the groups are those for whom the typical estimated TDEEs from the calculators have been shown to be less accurate on average makes this especially problematic (although assuming that estimated TDEE=real TDEE would be a problem in any case).
Yeah, I was being sarcastic in that last post. We were going round in circles. I think the issue was how we define underreporting. He keeps relating it to the formula and in my view, the formula has nothing to do with it. My definition of underreporting is when someone says/thinks/reports that they're eating X calories but in fact are eating more. Like an obese person saying they aren't losing on 1000 calories, which as we know, ends up being an error in measurements and mis-remembering what one ate.0 -
Traveler120 wrote: »lemurcat12 wrote: »Traveler120 wrote: »Ah ok, my bad. I mistakenly thought that 70% are overweight not because of inaccurate tdee equations, but because they eat too much (and underestimate intake) and exercise too little (and overestimate tdee). I stand corrected.
He wasn't saying that people gained weight due to inaccurate TDEE (or anything about how people gain weight). At least, that wasn't my interpretation. He was showing how TDEE estimates from the calculators may be misused, even in scientific studies--here to indicate underreporting by various groups of people. That in some of these cases the groups are those for whom the typical estimated TDEEs from the calculators have been shown to be less accurate on average makes this especially problematic (although assuming that estimated TDEE=real TDEE would be a problem in any case).
Yeah, I was being sarcastic in that last post. We were going round in circles. I think the issue was how we define underreporting. He keeps relating it to the formula and in my view, the formula has nothing to do with it. My definition of underreporting is when someone says/thinks/reports that they're eating X calories but in fact are eating more. Like an obese person saying they aren't losing on 1000 calories, which as we know, ends up being an error in measurements and mis-remembering what one ate.
Reporting here is actually writing down I ate x, y and z on a form as part of the study protocol. Under-reporting part is directly from the calculation of what was reported versus what the TDEE equation says they regularly eat.
It isn't about your definition, it is about the actual research protocol.
People may over-eating/"under-reporting" (as you define it) and still accurately reporting it into the study exactly but since the study is using a bias equation it will come out as "under reported" (actual reporting protocol).
People that are under weight or at weight (and according to you aren't "under reporting" since the are eating at maintenance and not obese) are as likely to under report diary entries or exercise events because these self-assessment protocols are faulty.
0 -
Oh I didn't realize that underreporting only occurs in a research study. Is it not possible to underreport intake on my mfp diary or other food log or to my friend? And when I'm filling in what I ate, do I need to know what my bmr or tdee is? No. It's simply understating what I ate. That's all I'm saying. Nothing more complicated than that. I'm not sure there's anything meaningful we're debating at this point other than restating what we already said.0
-
Traveler120 wrote: »lemurcat12 wrote: »Traveler120 wrote: »Ah ok, my bad. I mistakenly thought that 70% are overweight not because of inaccurate tdee equations, but because they eat too much (and underestimate intake) and exercise too little (and overestimate tdee). I stand corrected.
He wasn't saying that people gained weight due to inaccurate TDEE (or anything about how people gain weight). At least, that wasn't my interpretation. He was showing how TDEE estimates from the calculators may be misused, even in scientific studies--here to indicate underreporting by various groups of people. That in some of these cases the groups are those for whom the typical estimated TDEEs from the calculators have been shown to be less accurate on average makes this especially problematic (although assuming that estimated TDEE=real TDEE would be a problem in any case).
Yeah, I was being sarcastic in that last post. We were going round in circles. I think the issue was how we define underreporting.
I don't think that's the issue under discussion, is it? I thought the issue was the fact that BMR/TDEE calculated from the formulas was used to identify/define underreporting in certain studies. Those populations likely do underreport (as you would define it and me too -- report less than they eat), because MOST do, but the fact that they report eating less than their calculated TDEE doesn't prove that, and is arguably particularly poor evidence of it if the calculation/formula is more than usually inaccurate without [edit: within, I mean] their population group.0 -
Traveler120 wrote: »Oh I didn't realize that underreporting only occurs in a research study. Is it not possible to underreport intake on my mfp diary or other food log or to my friend? And when I'm filling in what I ate, do I need to know what my bmr or tdee is? No. It's simply understating what I ate. That's all I'm saying.
I see what's going on. EvgeniZyntx is talking about a research study, and you're talking about your opinion of what certain words mean. You should join the conversation everyone else is having. 0
0 -
Traveler120 wrote: »
Even from your graph, the widest point of variation is 1375 and 1475. That's only 100 calories. I don't know where you're getting 200 or more from your graph.EvgeniZyntx wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »ReaderGirl3 wrote: »CaptainJoy wrote: »Exercise is extremely important when in a calorie deficitbecause without it you can actually lower the rate you use calories while resting. This was proven by a U.S.government study done in 2009. Ci/co works but what good is losing the weight if you're just going to put it back on because you are no longer burning the same amount of calories at rest as you were before you lost the weight?
https://www.nia.nih.gov/newsroom/announcements/2009/05/study-shows-metabolic-adaptation-calorie-restriction
May I ask how long you've been in maintenance? 3 years into maintenance here, and I didn't exercise at all during my weight loss phase. My TDEE is spot on and has been since I started this whole thing back in 2012.
If you look at my profile it is obvious that I am not into maintenance "here." I did however lose 38 pounds about 28 years ago from diet and exercise and did a pretty good job of maintaining it until about 7 years ago. That would put me in maintenance for about 21 years. Of course that was before MFP. Exercise is important during weight loss to preserve our bone mass and metabolism as we get older. If you're happy and your TDEE is spot on then I'm happy for you. Not everyone is as lucky.
Yes, people keep telling my I'm a lucky freak of nature special snowflake TDEE calculators don't ask you your weight loss and exercise history. Many of us here have found these calculators to be very accurate, regardless of our dieting/exercise history. If not exercising during my weight loss phase had somehow lowered the rate I use calories while resting, then why would my TDEE still be accurate? From my own experience my TDEE is very accurate and it's what I go by now in maintenance. I haven't had any issues with my calorie amount being off.
These formulas are very rough estimators - here is an example graph of two leading formulas. If you find them accurate it is just confirmation bias. In every study they only correspond to about 65% of metabolic factors.
For example, consider women weighing 75Kg of different heights, you'll see that the equations only match at one point and may differ as much as 200 cals (or more).
From what I've read, the Mifflin St Jeor is widely regarded to be the most accurate.
I like the one posted by @ReaderGirl3 above. http://www.sailrabbit.com/bmr/. For me it's very accurate.
Best Ive seen.0 -
lemurcat12 wrote: »Gianfranco_R wrote: »lemurcat12 wrote: »The differences in TDEE calculators is going to be type of calculator (basically the main ones are Katch-McArdle, which uses BF%, Mifflin-St Jeor (what MFP uses for BMR and seemingly the most common), and Harris-Benedict).
For BMR, they give me (at goal of 120, assuming BF% of 22%, which makes sense with my most recent DEXA):
M-SJ=1155
H-B=1257
K-M=1289
I think BF% is the most accurate, so assuming I felt good about that measurement's accuracy, and did not have other numbers, I'd start with that.
Then the other variable is the activity factor. One way I've seen it is 1.2 for truly sedentary, 1.375 for lightly active, 1.5 or 1.55 for moderate, 1.725 for active, and 1.9 for extremely active.
Gives a wide range (more at higher levels of activity) and much room for error, for sure, which is why using your own numbers makes sense.
My own results (based on current weight of 125, not goal) is consistent with what the calculations would suggest for me. In that that doesn't mean much, as the range is so wide, I will say that what worked for me when I started seems to work now, in terms of estimating TDEE. I find the same calculators and estimates still seem to work (although the numbers are of course different).
It seems that most calculators on internet use that classification, but I would suggest to take a look at this document:
http://www.fao.org/3/a-y5686e.pdf
(see pages 37/38)
Okay, I have. Significantly higher. I wonder if that's because the numbers I quoted are more US-focused. The FAO report mentioned, for sedentary, someone living in a city with a sedentary job or a woman in African with a home-based business -- both likely to be more active than someone in the US who genuinely can drive everywhere in addition to having a sedentary job and may have lots of conveniences at home. I did find that even when I started and thought I was sedentary that my numbers were more like lightly active, which I attributed to living in a quite walkable big city and rarely driving. I'd think that's more like many Europeans (but who knows, I'm American so could be working on stereotypes).
I certainly would agree that the multiplier used and figuring out what it should be is a huge subjective factor. Lots of people think they are sedentary but aren't, and others probably think they are more active and aren't.
Thoughts?
Well, the FAO document is about proper nutrition, while those calculators that use the 1.2-1.9 range are probably "weight loss oriented" if I may say so.
To come back to the point where the tangent started, in my opinion it doesn't make sense to state that someone hasn't experienced metabolic adaptation because their TDEE is "spot on" with some calculators.0 -
Gianfranco_R wrote: »lemurcat12 wrote: »Gianfranco_R wrote: »lemurcat12 wrote: »The differences in TDEE calculators is going to be type of calculator (basically the main ones are Katch-McArdle, which uses BF%, Mifflin-St Jeor (what MFP uses for BMR and seemingly the most common), and Harris-Benedict).
For BMR, they give me (at goal of 120, assuming BF% of 22%, which makes sense with my most recent DEXA):
M-SJ=1155
H-B=1257
K-M=1289
I think BF% is the most accurate, so assuming I felt good about that measurement's accuracy, and did not have other numbers, I'd start with that.
Then the other variable is the activity factor. One way I've seen it is 1.2 for truly sedentary, 1.375 for lightly active, 1.5 or 1.55 for moderate, 1.725 for active, and 1.9 for extremely active.
Gives a wide range (more at higher levels of activity) and much room for error, for sure, which is why using your own numbers makes sense.
My own results (based on current weight of 125, not goal) is consistent with what the calculations would suggest for me. In that that doesn't mean much, as the range is so wide, I will say that what worked for me when I started seems to work now, in terms of estimating TDEE. I find the same calculators and estimates still seem to work (although the numbers are of course different).
It seems that most calculators on internet use that classification, but I would suggest to take a look at this document:
http://www.fao.org/3/a-y5686e.pdf
(see pages 37/38)
Okay, I have. Significantly higher. I wonder if that's because the numbers I quoted are more US-focused. The FAO report mentioned, for sedentary, someone living in a city with a sedentary job or a woman in African with a home-based business -- both likely to be more active than someone in the US who genuinely can drive everywhere in addition to having a sedentary job and may have lots of conveniences at home. I did find that even when I started and thought I was sedentary that my numbers were more like lightly active, which I attributed to living in a quite walkable big city and rarely driving. I'd think that's more like many Europeans (but who knows, I'm American so could be working on stereotypes).
I certainly would agree that the multiplier used and figuring out what it should be is a huge subjective factor. Lots of people think they are sedentary but aren't, and others probably think they are more active and aren't.
Thoughts?
Well, the FAO document is about proper nutrition, while those calculators that use the 1.2-1.9 range are probably "weight loss oriented" if I may say so.
To come back to the point where the tangent started, in my opinion it doesn't make sense to state that someone hasn't experienced metabolic adaptation because their TDEE is "spot on" with some calculators.
I doubt that's the difference.
With the calculators, if someone figured their TDEE using a particular method from the calculators and it worked and seemed to be roughly accurate and then used the same methodology after losing weight, I think that's decent evidence that there was not any significant metabolic adaptation.
Sure, who knows, but that gets to the point of what difference does it make anyway. My TDEE is normal for the amount of exercise I do (within a broad range of normal). Why should it matter to me if in some alternative universe where I never got fat it might be higher? The people who argue this matters posit that you are at some artificially low and unsustainable TDEE level after losing weight, and that's certainly not true -- and being within the normal range of the calculators is evidence that it is not.1 -
All I know is that dieting alone has never worked for me, it has to be a combination of cardio, strength training, and restricting calories while maintaining macros. I started looking at temptations like "thats going to be a whole extra 30 mins on the treadmill, and I don't have time for that." Plus i go on my lunch break so it really helps with appetite control, and when I get back and eat ny metabolism is fired up and I don't feel like a bottomless pit. I don't know why somebody wouldn't want to include exercise, I go from losing 1 pound a week to 3. Point I'm trying to make is that if it does nothing but change my mind frame about food that's enough reason to do it.2
-
Exercise is the reason I'm no longer anorexic. Exercise is a very important activity and beneficial for long-term fitness and results. I used to be very overweight and lost over 60 pounds by CICO alone with little to no exercise. In return I became anorexic, my energy was destroyed along with my appetite. After a year of being active again though (lifting weights, running, etc) my daily calorie allowance is larger, a lot of those skinny-fat spots are now solid/muscle, and my TDEE has increased. Calorie counting and losing weight without exercise = big mistake.3










This discussion has been closed.
Categories
- All Categories
- 1.4M Health, Wellness and Goals
- 398.2K Introduce Yourself
- 44.7K Getting Started
- 261K Health and Weight Loss
- 176.4K Food and Nutrition
- 47.7K Recipes
- 233K Fitness and Exercise
- 462 Sleep, Mindfulness and Overall Wellness
- 6.5K Goal: Maintaining Weight
- 8.7K Goal: Gaining Weight and Body Building
- 153.5K Motivation and Support
- 8.4K Challenges
- 1.4K Debate Club
- 96.5K Chit-Chat
- 2.6K Fun and Games
- 4.8K MyFitnessPal Information
- 12 News and Announcements
- 21 MyFitnessPal Academy
- 1.5K Feature Suggestions and Ideas
- 3.2K MyFitnessPal Tech Support Questions