Welcome to Debate Club! Please be aware that this is a space for respectful debate, and that your ideas will be challenged here. Please remember to critique the argument, not the author.
Do you think obese/overweight people should pay more for health insurance?
Replies
-
heiliskrimsli wrote: »If a smoker can be charged more, so should the overweight and obese.
True. I think it depends for sure but if it's someone who is obese then they will likely have health problems of some kind. It's kind of a null issue anyway if someone has insurance through their employer since all employees pay the same amount depending on their coverage choice.2 -
nevadavis1 wrote: »Also charging more just means that more overweight and obese people won't get health coverage and will not get preventative care and then won't see a doctor until they wind up in the ER with something life-threatening.
where I live most hospitals take in anyone regardless if they have insurance so they can pay it on a sliding scale or get assistance with paying their bill, not to mention Medicaid is offered in the USA.1 -
Should a person who makes choices that directly negatively affect their health be charged more for isurance. Absolutely. The choice could include, but not be limited to ... tobacco use, overeating to the point of morbid obesity, alcohol or drug abuse. If you purposely disregard your health then you should be penalized or taxed to compensate for it (I really like the tax idea that Japan does).
As a person who worked for a large health insurance company I carry a different perspective than someone who doesn't understand it. If you have an employer based insurance policy the employer is the one that dictates what they cover, not the insurance company. The insurance company follows the policy chosen by the employer and enforces it. If the employer chooses not to cover and experimental procedure then there is nothing you can do to force the insurance company to pay for it as it. As far as preexisting conditions, most policies waive that if there is no break in coverage from the previous policy to the current policy. If you've been years untreated for a condition and choose to pick up insurance just because you get pregnant or your condition worsens, why expect an insurance company to NOT see you as high risk and question your coverage. Once treated you could stop paying your coverage and the insurance company is left liable for thousands of medical bills when you only paid a few hundred dollars of premiums.3 -
As far as preexisting conditions, most policies waive that if there is no break in coverage from the previous policy to the current policy.
The ACA made it illegal to have pre-existing conditions be used for denial of coverage with the exception of very specific grandfathered plans regardless of breaks in coverage.0 -
Sure, let's charge overweight people more for their insurance, and while we are at it let's add smokers, heavy drinkers, those with high blood pressure, high cholesterol, or any congenital health condition. High cost has not deterred people from continuing to drink or smoke, what makes you think that the high cost of health insurance would be any different. Health costs are already sky high so let's make it even more affordable.0
-
@Sweets1954 smokers already pay more for life insurance, and cigarette taxes have drastically reduced smoking rates, especially in teens.5
-
Why is the emphasis on individual life style changes when other valid questions remain unaddressed. Why, for example is a hospital allowed to charge $100 for a Tylenol and $75 for a box of tissues? The reason health care facilities do not 'post' their fee schedule (as has been suggesting many times) is because the Registrar will investigate what a patient's individual policy will allow, and charge accordingly. How convenient for hospitals, insurers, Pharma, medical device suppliers, etc that the conversion continues to encourage the policyholders to focus on dividing and blaming each other. #allroadsleadtoasinglepayer
And by the way, if anyone can point me to a country that provides universal health care where the citizenry is lobbying their government to end the madness and take up a 'great' system like we have here is US, I would gladly look into their reasons.8 -
armchairherpetologist wrote: »As far as preexisting conditions, most policies waive that if there is no break in coverage from the previous policy to the current policy.
The ACA made it illegal to have pre-existing conditions be used for denial of coverage with the exception of very specific grandfathered plans regardless of breaks in coverage.
We all see how well AHA has worked haven't we?1 -
Why is the emphasis on individual life style changes when other valid questions remain unaddressed. Why, for example is a hospital allowed to charge $100 for a Tylenol and $75 for a box of tissues? The reason health care facilities do not 'post' their fee schedule (as has been suggesting many times) is because the Registrar will investigate what a patient's individual policy will allow, and charge accordingly. How convenient for hospitals, insurers, Pharma, medical device suppliers, etc that the conversion continues to encourage the policyholders to focus on dividing and blaming each other. #allroadsleadtoasinglepayer
And by the way, if anyone can point me to a country that provides universal health care where the citizenry is lobbying their government to end the madness and take up a 'great' system like we have here is US, I would gladly look into their reasons.
Physician and facilities can charge whatever they want but are contractually obligated to accept the fee schedules designated by the heath insurance ... that where your participate vs non participating providers come into play. The part that most people don't realize is that the amount over the insurance companies fee schedule are actually a tax write off for the provider. Example ... hospital charges $7000 for a maternity claim, insurance determine only $3000 allowed and benefits are paid based on that. The remaining $4000 is a tax write off for the hospital.
2 -
Why is the emphasis on individual life style changes when other valid questions remain unaddressed. Why, for example is a hospital allowed to charge $100 for a Tylenol and $75 for a box of tissues? The reason health care facilities do not 'post' their fee schedule (as has been suggesting many times) is because the Registrar will investigate what a patient's individual policy will allow, and charge accordingly. How convenient for hospitals, insurers, Pharma, medical device suppliers, etc that the conversion continues to encourage the policyholders to focus on dividing and blaming each other. #allroadsleadtoasinglepayer
And by the way, if anyone can point me to a country that provides universal health care where the citizenry is lobbying their government to end the madness and take up a 'great' system like we have here is US, I would gladly look into their reasons.
Government is one of the root causes of the problem...and your solution is to grant them all the power?2 -
I'm with you.SoulRadiation wrote: »I think it would be more logical to do away with the private insurance industry, have national healthcare, and provide tax incentives for living well (healthy weight, non-smoking, etc)...and do so under the justification that this is done to promote the common welfare.
The VA has a different set of pros and cons than private insurance. My personal list:MonaLisaLianne wrote: »Because we can see what a wonderful job the one-payer system called the Veteran's Administration has done in providing health care?- I like getting a LOT more time with my providers than I did when in an HMO.
- I don't like having to commute into Boston for an ultrasound or to see a dermatologist.
- I don't have long wait times here in MA, and the only time I had long wait times in FL was for an ultrasound, and that was before the VA Choice program.
- I like that everything is coordinated and all my providers can see my records.
- I don't the bureaucracy that creates inefficiency and necessitates multiple visits.
Interesting idea.richardgavel wrote: »I'm not in favor of single payer, but the VA issue is not really one of single payer. Rather it's single PROVIDER. The two are not necessarily mutually linked. Personally I wish VA would be more like Medicare, the entity that pays the bills and a smaller medical VA that might specialize in medical issues unique to service members and leave more standard stuff to standard providers.
4 -
Sweets1954 wrote: »Sure, let's charge overweight people more for their insurance, and while we are at it let's add smokers, heavy drinkers, those with high blood pressure, high cholesterol, or any congenital health condition. High cost has not deterred people from continuing to drink or smoke, what makes you think that the high cost of health insurance would be any different. Health costs are already sky high so let's make it even more affordable.
It would be a nice bonus if charging obese people more made them change their ways, but they should be charged more even if it doesn't have that effect. The bottom line is that if you DON"T charge the obese more, people at a healthy weight pay more to subsidize the obese. That is fundamentally unfair. Why should I pay more to subsidize somebody else's unhealthy lifestyle?
If obese people paid an amount that was appropriate for their high risk lifestyle, other people could pay less. That would be a good outcome.4 -
Alatariel75 wrote: »... I'm so glad I live in Australia.
The current US president agrees that Australia's universal health care is better that what we in the US have.2 -
Why is the emphasis on individual life style changes when other valid questions remain unaddressed. Why, for example is a hospital allowed to charge $100 for a Tylenol and $75 for a box of tissues? The reason health care facilities do not 'post' their fee schedule (as has been suggesting many times) is because the Registrar will investigate what a patient's individual policy will allow, and charge accordingly. How convenient for hospitals, insurers, Pharma, medical device suppliers, etc that the conversion continues to encourage the policyholders to focus on dividing and blaming each other. #allroadsleadtoasinglepayer
And by the way, if anyone can point me to a country that provides universal health care where the citizenry is lobbying their government to end the madness and take up a 'great' system like we have here is US, I would gladly look into their reasons.
Physician and facilities can charge whatever they want but are contractually obligated to accept the fee schedules designated by the heath insurance ... that where your participate vs non participating providers come into play. The part that most people don't realize is that the amount over the insurance companies fee schedule are actually a tax write off for the provider. Example ... hospital charges $7000 for a maternity claim, insurance determine only $3000 allowed and benefits are paid based on that. The remaining $4000 is a tax write off for the hospital.
I don't think that is the case. The hospital made a contractual agreement with the responsible party (the insured and his/her insurance company) to accept an amount less than the standard price (sticker price). That would not be a tax write-off.
A car dealer doesn't get a tax write-off for the difference if he sells a car to someone for less than the sticker price.
0 -
I am suggesting we take a more holistic approach to the problems instead of just targeting the insurance dynamic. There's plenty of other places to search for improvements besides the individual consumer1
-
@N6314P what do you have in mind?0
-
Packerjohn wrote: »Why is the emphasis on individual life style changes when other valid questions remain unaddressed. Why, for example is a hospital allowed to charge $100 for a Tylenol and $75 for a box of tissues? The reason health care facilities do not 'post' their fee schedule (as has been suggesting many times) is because the Registrar will investigate what a patient's individual policy will allow, and charge accordingly. How convenient for hospitals, insurers, Pharma, medical device suppliers, etc that the conversion continues to encourage the policyholders to focus on dividing and blaming each other. #allroadsleadtoasinglepayer
And by the way, if anyone can point me to a country that provides universal health care where the citizenry is lobbying their government to end the madness and take up a 'great' system like we have here is US, I would gladly look into their reasons.
Physician and facilities can charge whatever they want but are contractually obligated to accept the fee schedules designated by the heath insurance ... that where your participate vs non participating providers come into play. The part that most people don't realize is that the amount over the insurance companies fee schedule are actually a tax write off for the provider. Example ... hospital charges $7000 for a maternity claim, insurance determine only $3000 allowed and benefits are paid based on that. The remaining $4000 is a tax write off for the hospital.
I don't think that is the case. The hospital made a contractual agreement with the responsible party (the insured and his/her insurance company) to accept an amount less than the standard price (sticker price). That would not be a tax write-off.
A car dealer doesn't get a tax write-off for the difference if he sells a car to someone for less than the sticker price.
Actually it's exactly the case. I worked for a prominent nationwide health insurance company for almost 10 years and the providers (providers being both physicians and facilities) are very aware of the tax deduction process. Charges not paid that exceed the MAC (maximum allowable charge) are tax deduction while charges denied as say non covered are not. Non covered makes it the patients responsibility while exceeding the MAC makes it the providers responsibility ... whereas making it a loss to be claimed as a tax deduction.
In your example of a car dealership it would be considered a loss if he sold it for less than his purchase price. He would be allowed go use it as a tax deduction if he took a loss on it.4 -
richardgavel wrote: »To those who don't want the obese to pay more, are you willing to make up the difference? Are you ready to fork over more money for your own insurance, since obesity is resulting in higher health care costs, in the name of keeping everyone's insurance costs the same?
I'd like the US to switch to single payer and pay for it by decreasing spending on war.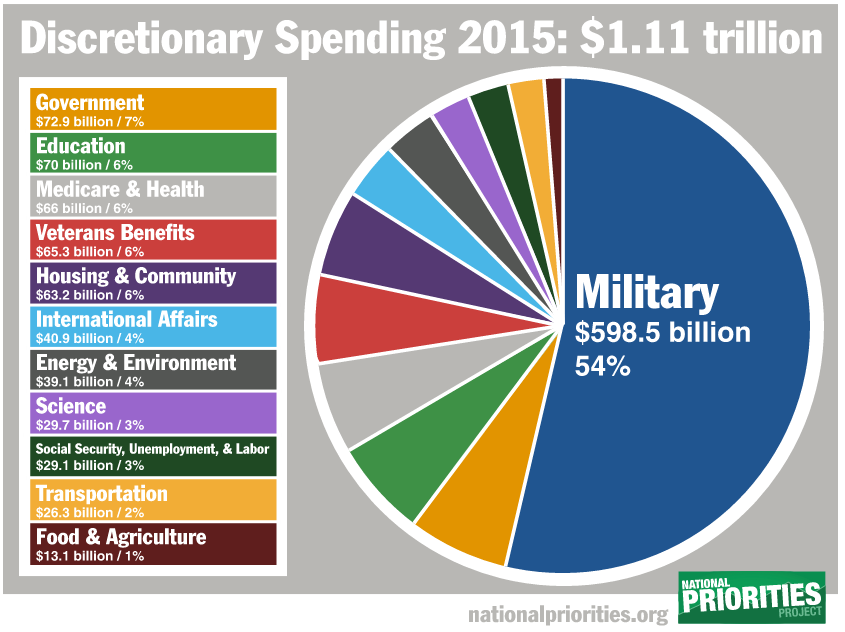
https://www.nationalpriorities.org/
This is how the United States budget allocates $1.11 trillion in discretionary spending in fiscal year 2015. Discretionary spending, which accounts for 29 percent of the total 2015 budget, includes programs whose funding levels are set each year by lawmakers during the appropriations process, including the military, education, job training, and the environment. It does not include earned-benefit programs like Social Security and Medicare. See our Total Spending chart to see how the full $3.84 trillion federal budget will be spent in 2015.
7 -
kshama2001 wrote: »
I'm with you.SoulRadiation wrote: »I think it would be more logical to do away with the private insurance industry, have national healthcare, and provide tax incentives for living well (healthy weight, non-smoking, etc)...and do so under the justification that this is done to promote the common welfare.
The VA has a different set of pros and cons than private insurance. My personal list:MonaLisaLianne wrote: »Because we can see what a wonderful job the one-payer system called the Veteran's Administration has done in providing health care?- I like getting a LOT more time with my providers than I did when in an HMO.
- I don't like having to commute into Boston for an ultrasound or to see a dermatologist.
- I don't have long wait times here in MA, and the only time I had long wait times in FL was for an ultrasound, and that was before the VA Choice program.
- I like that everything is coordinated and all my providers can see my records.
- I don't the bureaucracy that creates inefficiency and necessitates multiple visits.
Interesting idea.richardgavel wrote: »I'm not in favor of single payer, but the VA issue is not really one of single payer. Rather it's single PROVIDER. The two are not necessarily mutually linked. Personally I wish VA would be more like Medicare, the entity that pays the bills and a smaller medical VA that might specialize in medical issues unique to service members and leave more standard stuff to standard providers.
The VA is a single-payer system. All the bills are paid for by the taxpayer. All providers, all services, all materials and equipment are paid for by Uncle Sam.
The VA is interesting. Typically patients enrolled in VA care and receiving treatment report high satisfaction with their providers and care (with some exceptions). However, the rub is that in order to get VA care, you need to be 1) eligible for care and 2) enrolled in the VA and 3) satisfy the means-testing and disability-rating process in order to receive services (depending on the service).
This basically translates into the VA being the most highly managed, managed-care system on earth. Once you're enrolled and 100% service connected, you do pretty darn good, everything is "free." But you need to go through mountains of red tape and waiting lists to get there.
(I know all of this in intimate detail - don't ask why)5 -
If we let insurance companies charge more for MFP participation, is it Chit-Chat or Fun and Games that get the most points for that kind of risky behavior? And does it outweigh the increased risk of hypertension for worrying about people being wrong in Debate? ;-)7
-
Well of course, it just makes sense. It would also give more motivation to improve their health. Our current system basically rewards people letting themselves go. Yeah they might die at 35 from complications with diabetes but that doesn't seem like motivation for most.3
-
Sweets1954 wrote: »Sure, let's charge overweight people more for their insurance, and while we are at it let's add smokers, heavy drinkers, those with high blood pressure, high cholesterol, or any congenital health condition. High cost has not deterred people from continuing to drink or smoke, what makes you think that the high cost of health insurance would be any different. Health costs are already sky high so let's make it even more affordable.
And don't forget people with revolving sex partners and their many close calls with cooties.
It is possible to have a lot of partners and never have a close call. Not even what I'd call diffi,based on experience.0 -
armchairherpetologist wrote: »Sweets1954 wrote: »Sure, let's charge overweight people more for their insurance, and while we are at it let's add smokers, heavy drinkers, those with high blood pressure, high cholesterol, or any congenital health condition. High cost has not deterred people from continuing to drink or smoke, what makes you think that the high cost of health insurance would be any different. Health costs are already sky high so let's make it even more affordable.
And don't forget people with revolving sex partners and their many close calls with cooties.
It is possible to have a lot of partners and never have a close call. Not even what I'd call diffi,based on experience.
Oh sure. That's what they all say.
Unless you have no standards, an aversion to testing, and refuse to use protection, it's not like everyone with more than one partner is a walking Petri dish.
It is even quite possible to enjoy the sport of one-nighters and not be a disease factory. But many like to judge those with ore permissive sexual attitudes, and throwing around "diseased" is a pretty typical way.2 -
VintageFeline wrote: »Packerjohn wrote: »IMO, until the US healthcare system isn't a FOR PROFIT venture, people will end up spending their retirement income and savings on it. See how much it costs to get hospitalized or how much medication costs for people who need it. It's pretty astounding and outrageous.
We could pay for ALL AMERICANS healthcare, it's just that our government chooses to spend more of taxes towards the military might instead.
A.C.E. Certified Personal and Group Fitness Trainer
IDEA Fitness member
Kickboxing Certified Instructor
Been in fitness for 30 years and have studied kinesiology and nutrition
The issue with health care in the US is spending per person (from all sources) is doube what it is for the rest of the industrialized world.
Profit is a portion of this but nowhere near all. I believe one of our issues is the amont we spend on end of life care. Most other countries will make an 80 year with a serious illness comfortable and leto them die with no treatment. In the US we spend thousands of dollars for an extra couple of months of life with questionable quality.
I'm in the UK. We most certainly do not leave 80 year olds to die. There are people in their late 80s having surgeries that may extend life for just a few months or a few years. Everyone gets healthcare equally if it's approved by NICE (they control what treatments the NHS will pay for, such as new cancer drugs but it's applied almost universally with a little postcode lottery thrown in).
And these types of conversations terrify me coming from a country with nationalised healthcare. Our doctors don't prescribe medications because they'll get a kickback. They don't meet pharmaceutical salesmen who again, offer incentives to use their medications.
You get treatment based purely on medical need and what is appropriate to the individual. There's no yearly health check (unless you do have private healthcare, which is available if you have the money for it but it feels for the most part, another way to make some money).
Our government are doing their best to privatise our healthcare by stealth by chronically underfunding and then pointing fingers at mismanagement etc in order to do so.
I have chronic health conditions, I will probably be on medication for life. When I see the costs some pay for my medication I know I couldn't afford even a fraction of that. So then what for those people? They cost the country more for being medically unfit for anything than if they were just allowed access to treatment.
I'm in the UK and in the same position. I'm on a new medication which has kept me well for over a year and each time I read (on support forums elsewhere) of people in my situation in America being denied medication or having to tie their house to debts, I am hugely grateful for our NHS.
Having said that,even in the UK funding decisions are made based partly on people's "lifestyle choices ". In order to get funding for my medication I had to demonstrate compliance with previous medication plans. I was asked questions about smoking and drinking habits. And NICE guidelines are partly based on costs.2 -
kshama2001 wrote: »
I'm with you.SoulRadiation wrote: »I think it would be more logical to do away with the private insurance industry, have national healthcare, and provide tax incentives for living well (healthy weight, non-smoking, etc)...and do so under the justification that this is done to promote the common welfare.
The VA has a different set of pros and cons than private insurance. My personal list:MonaLisaLianne wrote: »Because we can see what a wonderful job the one-payer system called the Veteran's Administration has done in providing health care?- I like getting a LOT more time with my providers than I did when in an HMO.
- I don't like having to commute into Boston for an ultrasound or to see a dermatologist.
- I don't have long wait times here in MA, and the only time I had long wait times in FL was for an ultrasound, and that was before the VA Choice program.
- I like that everything is coordinated and all my providers can see my records.
- I don't the bureaucracy that creates inefficiency and necessitates multiple visits.
Interesting idea.richardgavel wrote: »I'm not in favor of single payer, but the VA issue is not really one of single payer. Rather it's single PROVIDER. The two are not necessarily mutually linked. Personally I wish VA would be more like Medicare, the entity that pays the bills and a smaller medical VA that might specialize in medical issues unique to service members and leave more standard stuff to standard providers.
The VA is a single-payer system. All the bills are paid for by the taxpayer. All providers, all services, all materials and equipment are paid for by Uncle Sam.
The VA is interesting. Typically patients enrolled in VA care and receiving treatment report high satisfaction with their providers and care (with some exceptions). However, the rub is that in order to get VA care, you need to be 1) eligible for care and 2) enrolled in the VA and 3) satisfy the means-testing and disability-rating process in order to receive services (depending on the service).
This basically translates into the VA being the most highly managed, managed-care system on earth. Once you're enrolled and 100% service connected, you do pretty darn good, everything is "free." But you need to go through mountains of red tape and waiting lists to get there.
(I know all of this in intimate detail - don't ask why)
The VA is an excellent example of the ultimate endpoint of all socialized structures. I should be able to get nearly all my care through the VA; however due to the waiting lines and structure this system makes me holding a job and receiving care impossible.
For the few instances I've utilized the VA - outstanding service. The medical staff are top notch and as many are veterans there is a common bond which enhances the bedside manner and relationship between caregiver and patient. Getting care is the issue and since you have limited resources and unlimited demand you have to ration. A teammate documented his attempts to get care for severe pain connected to a service related injury - he waited for an initial examination six months.
The key difference is that with the VA there is a connection to service. This does not exist in single payer, so any issues you find with the VA will be compounded exponentially.4 -
kshama2001 wrote: »
I'm with you.SoulRadiation wrote: »I think it would be more logical to do away with the private insurance industry, have national healthcare, and provide tax incentives for living well (healthy weight, non-smoking, etc)...and do so under the justification that this is done to promote the common welfare.
The VA has a different set of pros and cons than private insurance. My personal list:MonaLisaLianne wrote: »Because we can see what a wonderful job the one-payer system called the Veteran's Administration has done in providing health care?- I like getting a LOT more time with my providers than I did when in an HMO.
- I don't like having to commute into Boston for an ultrasound or to see a dermatologist.
- I don't have long wait times here in MA, and the only time I had long wait times in FL was for an ultrasound, and that was before the VA Choice program.
- I like that everything is coordinated and all my providers can see my records.
- I don't the bureaucracy that creates inefficiency and necessitates multiple visits.
Interesting idea.richardgavel wrote: »I'm not in favor of single payer, but the VA issue is not really one of single payer. Rather it's single PROVIDER. The two are not necessarily mutually linked. Personally I wish VA would be more like Medicare, the entity that pays the bills and a smaller medical VA that might specialize in medical issues unique to service members and leave more standard stuff to standard providers.
The VA is a single-payer system. All the bills are paid for by the taxpayer. All providers, all services, all materials and equipment are paid for by Uncle Sam.
The VA is interesting. Typically patients enrolled in VA care and receiving treatment report high satisfaction with their providers and care (with some exceptions). However, the rub is that in order to get VA care, you need to be 1) eligible for care and 2) enrolled in the VA and 3) satisfy the means-testing and disability-rating process in order to receive services (depending on the service).
This basically translates into the VA being the most highly managed, managed-care system on earth. Once you're enrolled and 100% service connected, you do pretty darn good, everything is "free." But you need to go through mountains of red tape and waiting lists to get there.
(I know all of this in intimate detail - don't ask why)
The VA is an excellent example of the ultimate endpoint of all socialized structures. I should be able to get nearly all my care through the VA; however due to the waiting lines and structure this system makes me holding a job and receiving care impossible.
For the few instances I've utilized the VA - outstanding service. The medical staff are top notch and as many are veterans there is a common bond which enhances the bedside manner and relationship between caregiver and patient. Getting care is the issue and since you have limited resources and unlimited demand you have to ration. A teammate documented his attempts to get care for severe pain connected to a service related injury - he waited for an initial examination six months.
The key difference is that with the VA there is a connection to service. This does not exist in single payer, so any issues you find with the VA will be compounded exponentially.
Given my experience in Miami and Boston, I believe problems with wait times in the VA are due to regional understaffing, not a problem with the system as a whole.
Also, since the scandal about wait times in Phoenix, they've been aggressive about scheduling me for appointments I'm not even ready to schedule.4 -
Sweets1954 wrote: »Sure, let's charge overweight people more for their insurance, and while we are at it let's add smokers, heavy drinkers, those with high blood pressure, high cholesterol, or any congenital health condition. High cost has not deterred people from continuing to drink or smoke, what makes you think that the high cost of health insurance would be any different. Health costs are already sky high so let's make it even more affordable.
And don't forget people with revolving sex partners and their many close calls with cooties.
Why? How do you expect your medical insurance to deal with that?1 -
kshama2001 wrote: »I'd like the US to switch to single payer and pay for it by decreasing spending on war.
That's not going to happen. It's just as realistic to say we should just "print" enough money to treat everybody. After all, money isn't a finite resource, we haven't reached full employment, and there's no critical drug shortage. These are both pie-in-the-sky ideas.1 -
kshama2001 wrote: »kshama2001 wrote: »
I'm with you.SoulRadiation wrote: »I think it would be more logical to do away with the private insurance industry, have national healthcare, and provide tax incentives for living well (healthy weight, non-smoking, etc)...and do so under the justification that this is done to promote the common welfare.
The VA has a different set of pros and cons than private insurance. My personal list:MonaLisaLianne wrote: »Because we can see what a wonderful job the one-payer system called the Veteran's Administration has done in providing health care?- I like getting a LOT more time with my providers than I did when in an HMO.
- I don't like having to commute into Boston for an ultrasound or to see a dermatologist.
- I don't have long wait times here in MA, and the only time I had long wait times in FL was for an ultrasound, and that was before the VA Choice program.
- I like that everything is coordinated and all my providers can see my records.
- I don't the bureaucracy that creates inefficiency and necessitates multiple visits.
Interesting idea.richardgavel wrote: »I'm not in favor of single payer, but the VA issue is not really one of single payer. Rather it's single PROVIDER. The two are not necessarily mutually linked. Personally I wish VA would be more like Medicare, the entity that pays the bills and a smaller medical VA that might specialize in medical issues unique to service members and leave more standard stuff to standard providers.
The VA is a single-payer system. All the bills are paid for by the taxpayer. All providers, all services, all materials and equipment are paid for by Uncle Sam.
The VA is interesting. Typically patients enrolled in VA care and receiving treatment report high satisfaction with their providers and care (with some exceptions). However, the rub is that in order to get VA care, you need to be 1) eligible for care and 2) enrolled in the VA and 3) satisfy the means-testing and disability-rating process in order to receive services (depending on the service).
This basically translates into the VA being the most highly managed, managed-care system on earth. Once you're enrolled and 100% service connected, you do pretty darn good, everything is "free." But you need to go through mountains of red tape and waiting lists to get there.
(I know all of this in intimate detail - don't ask why)
The VA is an excellent example of the ultimate endpoint of all socialized structures. I should be able to get nearly all my care through the VA; however due to the waiting lines and structure this system makes me holding a job and receiving care impossible.
For the few instances I've utilized the VA - outstanding service. The medical staff are top notch and as many are veterans there is a common bond which enhances the bedside manner and relationship between caregiver and patient. Getting care is the issue and since you have limited resources and unlimited demand you have to ration. A teammate documented his attempts to get care for severe pain connected to a service related injury - he waited for an initial examination six months.
The key difference is that with the VA there is a connection to service. This does not exist in single payer, so any issues you find with the VA will be compounded exponentially.
Given my experience in Miami and Boston, I believe problems with wait times in the VA are due to regional understaffing, not a problem with the system as a whole.
Also, since the scandal about wait times in Phoenix, they've been aggressive about scheduling me for appointments I'm not even ready to schedule.
I was stationed at Dam Neck and utilized Portsmouth VA after initial separation and had no issues. I currently use North Chicago, which is a cluster - all administration and no front lines. My next door neighbor is a RN working there and just frustrated with all the poor admin decisions. Budgets are always approved for new meeting rooms, new TV displays, non-essentials for the administrators yet her department is scrounging for medical necessities.
My teammate lives just outside of Phoenix. He travels a lot and offered to use a different network and his request went unanswered.0 -
No0











This discussion has been closed.
Categories
- All Categories
- 1.4M Health, Wellness and Goals
- 398.4K Introduce Yourself
- 44.7K Getting Started
- 261K Health and Weight Loss
- 176.4K Food and Nutrition
- 47.7K Recipes
- 233K Fitness and Exercise
- 462 Sleep, Mindfulness and Overall Wellness
- 6.5K Goal: Maintaining Weight
- 8.7K Goal: Gaining Weight and Body Building
- 153.5K Motivation and Support
- 8.4K Challenges
- 1.4K Debate Club
- 96.5K Chit-Chat
- 2.6K Fun and Games
- 4.7K MyFitnessPal Information
- 17 News and Announcements
- 21 MyFitnessPal Academy
- 1.5K Feature Suggestions and Ideas
- 3.2K MyFitnessPal Tech Support Questions