Thought I'd picked a healthy breakfast option ...
Replies
-
I think this abstract sums up the sources of my frustrated confusion on the issue. Note how they know what happens in rats, but humans seem to have different reactions, and they don't know what long term lower sugar consumption is going to do to us even though short term higher consumption does increase intrahepatic fat concentration. But also note that they mention moderate amounts as %10 of energy intake in the US and Europe. In 2010, teens and children were getting %16 of calories from added sugar. (source: http://www.cdc.gov/nchs/data/databriefs/db122.htm). I'm fascinated with the subject, and I want my liver to last a very long time, but there is a lot of contradictory information out there.
Summary
Fructose is mainly consumed with added sugars (sucrose and high fructose corn syrup), and represents up to 10% of total energy intake in the US and in several European countries. This hexose is essentially metabolized in splanchnic tissues, where it is converted into glucose, glycogen, lactate, and, to a minor extent, fatty acids. In animal models, high fructose diets cause the development of obesity, insulin resistance, diabetes mellitus, and dyslipidemia. Ectopic lipid deposition in the liver is an early occurrence upon fructose exposure, and is tightly linked to hepatic insulin resistance. In humans, there is strong evidence, based on several intervention trials, that fructose overfeeding increases fasting and postprandial plasma triglyceride concentrations, which are related to stimulation of hepatic de novo lipogenesis and VLDL-TG secretion, together with decreased VLDL-TG clearance. However, in contrast to animal models, fructose intakes as high as 200 g/day in humans only modestly decreases hepatic insulin sensitivity, and has no effect on no whole body (muscle) insulin sensitivity. A possible explanation may be that insulin resistance and dysglycemia develop mostly in presence of sustained fructose exposures associated with changes in body composition. Such effects are observed with high daily fructose intakes, and there is no solid evidence that fructose, when consumed in moderate amounts, has deleterious effects. There is only limited information regarding the effects of fructose on intrahepatic lipid concentrations. In animal models, high fructose diets clearly stimulate hepatic de novo lipogenesis and cause hepatic steatosis. In addition, some observations suggest that fructose may trigger hepatic inflammation and stimulate the development of hepatic fibrosis. This raises the possibility that fructose may promote the progression of non-alcoholic fatty liver disease to its more severe forms, i.e. non-alcoholic steatohepatitis and cirrhosis. In humans, a short-term fructose overfeeding stimulates de novo lipogenesis and significantly increases intrahepatic fat concentration, without however reaching the proportion encountered in non-alcoholic fatty liver diseases. Whether consumption of lower amounts of fructose over prolonged periods may contribute to the pathogenesis of NAFLD has not been convincingly documented in epidemiological studies and remains to be further assessed.
http://www.sciencedirect.com/science/article/pii/S2210740112001866
LOL "Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). The survey consists of interviews conducted in participants' homes, standardized physical examinations in mobile examination centers (MECs), and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination. Dietary information for this analysis was obtained via an in-person 24-hour dietary recall interview in the MEC."
and lol at your abstract, how many people are consuming over 200g of fructose a day? And animal models? I wonder if DNL occurs at similar rates as humans or it's much much different?
There are other studies, including small scale human ones. I deliberately picked one that is difficult to read (as far as the abstract goes) and contradictory.
But since you don't like that one, let's have a human one:
http://www.mdpi.com/2072-6643/6/8/3187/htm
Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD
Abstract: Nonalcoholic fatty liver disease (NAFLD) is now thought to be the most common liver disease worldwide. Cardiovascular complications are a leading cause of mortality in NAFLD. Fructose, a common nutrient in the westernized diet, has been reported to be associated with increased cardiovascular risk, but its impact on adolescents with NAFLD is not well understood. We designed a 4-week randomized, controlled, double-blinded beverage intervention study. Twenty-four overweight Hispanic-American adolescents who had hepatic fat >8% on imaging and who were regular consumers of sweet beverages were enrolled and randomized to calorie-matched study-provided fructose only or glucose only beverages. After 4 weeks, there was no significant change in hepatic fat or body weight in either group. In the glucose beverage group there was significantly improved adipose insulin sensitivity, high sensitivity C-reactive protein (hs-CRP), and low-density lipoprotein (LDL) oxidation. These findings demonstrate that reduction of fructose improves several important factors related to cardiovascular disease despite a lack of measurable improvement in hepatic steatosis. Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials.
This one, too:
http://onlinelibrary.wiley.com/doi/10.1002/hep.26299/full
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in adults and children. A number of genetic and environmental factors are known to predispose individuals to NAFLD. Certain dietary sugars, particularly fructose, are suspected to contribute to the development of NAFLD and its progression. The increasing quantity of fructose in the diet comes from sugar additives (most commonly sucrose and high fructose corn syrup) in beverages and processed foods. Substantial links have been demonstrated between increased fructose consumption and obesity, dyslipidemia, and insulin resistance. Growing evidence suggests that fructose contributes to the development and severity of NAFLD. In human studies, fructose is associated with increasing hepatic fat, inflammation, and possibly fibrosis. Whether fructose alone can cause NAFLD or if it serves only as a contributor when consumed excessively in the setting of insulin resistance, positive energy balance, and sedentary lifestyle is unknown. Sufficient evidence exists to support clinical recommendations that fructose intake be limited through decreasing foods and drinks high in added (fructose-containing) sugars. (Hepatology 2013;57:2525–2531)
How many do you want?
0 -
Am I mistaken, or did some people write that they think refined sugar is good for you??0
-
"Being good for you" and "not hurting in moderation" are different things. I eat within my sugar macros, because I like sugar and it's tasty. Live a little. Also I don't have health problems concerning sugar. Are you going to say "not yet"?
") 0
0 -
Am I mistaken, or did some people write that they think refined sugar is good for you??
the argument being made is that one food group or macro nutrient is not bad for you. What matters is overall diet and dosage. You can eat sugar in the context of an overall diet where macro and micro needs are met and you hit your calorie goal.
sugar is not inherently bad.0 -
-
A good diet recommends about 45-50 % of daily calories allowed from Total carbs
Some carbs like sugar is 100 sugar. You can either eat sugar and get the target but will miss out on fullness, fibre vitamins amd minerals. Choose Carbs with low sugar and you have a healthy filling meal !
Jit0 -
You're right to be surprised to find so much sugar. You would've thought it should be maybe half that amount, right? I am not a fan that plain, non-fat yogurt has 15 g of sugar...and it's not sweet at all! There's naturally a decent amount of sugar in milk. So yeah, yogurt is kinda high sugar. I shoot for under 10 g of sugar regardless of whether it's a meal or snack. So I'm considering switching out my plain yogurt for non-fat cottage cheese...maybe not the most popular dairy product in the world, but the sugar is at least half the amount of yogurt and maintains the high protein (might even have more). Not that you want cottage cheese for breakfast, but if you can stand the thought, consider switching it out too.0
-
The name lies - greek "yogurt" is better at passing for sour cream. Get unsweetened stuff next time and pile it on some potatoes. Or use it in stroganoff. Or add onion soup mix and dip things in it. Just please don't add sugary things to it - it's a healthy food but it doesn't lend itself well to that.0
-
I think this abstract sums up the sources of my frustrated confusion on the issue. Note how they know what happens in rats, but humans seem to have different reactions, and they don't know what long term lower sugar consumption is going to do to us even though short term higher consumption does increase intrahepatic fat concentration. But also note that they mention moderate amounts as %10 of energy intake in the US and Europe. In 2010, teens and children were getting %16 of calories from added sugar. (source: http://www.cdc.gov/nchs/data/databriefs/db122.htm). I'm fascinated with the subject, and I want my liver to last a very long time, but there is a lot of contradictory information out there.
Summary
Fructose is mainly consumed with added sugars (sucrose and high fructose corn syrup), and represents up to 10% of total energy intake in the US and in several European countries. This hexose is essentially metabolized in splanchnic tissues, where it is converted into glucose, glycogen, lactate, and, to a minor extent, fatty acids. In animal models, high fructose diets cause the development of obesity, insulin resistance, diabetes mellitus, and dyslipidemia. Ectopic lipid deposition in the liver is an early occurrence upon fructose exposure, and is tightly linked to hepatic insulin resistance. In humans, there is strong evidence, based on several intervention trials, that fructose overfeeding increases fasting and postprandial plasma triglyceride concentrations, which are related to stimulation of hepatic de novo lipogenesis and VLDL-TG secretion, together with decreased VLDL-TG clearance. However, in contrast to animal models, fructose intakes as high as 200 g/day in humans only modestly decreases hepatic insulin sensitivity, and has no effect on no whole body (muscle) insulin sensitivity. A possible explanation may be that insulin resistance and dysglycemia develop mostly in presence of sustained fructose exposures associated with changes in body composition. Such effects are observed with high daily fructose intakes, and there is no solid evidence that fructose, when consumed in moderate amounts, has deleterious effects. There is only limited information regarding the effects of fructose on intrahepatic lipid concentrations. In animal models, high fructose diets clearly stimulate hepatic de novo lipogenesis and cause hepatic steatosis. In addition, some observations suggest that fructose may trigger hepatic inflammation and stimulate the development of hepatic fibrosis. This raises the possibility that fructose may promote the progression of non-alcoholic fatty liver disease to its more severe forms, i.e. non-alcoholic steatohepatitis and cirrhosis. In humans, a short-term fructose overfeeding stimulates de novo lipogenesis and significantly increases intrahepatic fat concentration, without however reaching the proportion encountered in non-alcoholic fatty liver diseases. Whether consumption of lower amounts of fructose over prolonged periods may contribute to the pathogenesis of NAFLD has not been convincingly documented in epidemiological studies and remains to be further assessed.
http://www.sciencedirect.com/science/article/pii/S2210740112001866
LOL "Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). The survey consists of interviews conducted in participants' homes, standardized physical examinations in mobile examination centers (MECs), and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination. Dietary information for this analysis was obtained via an in-person 24-hour dietary recall interview in the MEC."
and lol at your abstract, how many people are consuming over 200g of fructose a day? And animal models? I wonder if DNL occurs at similar rates as humans or it's much much different?
There are other studies, including small scale human ones. I deliberately picked one that is difficult to read (as far as the abstract goes) and contradictory.
But since you don't like that one, let's have a human one:
http://www.mdpi.com/2072-6643/6/8/3187/htm
Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD
Abstract: Nonalcoholic fatty liver disease (NAFLD) is now thought to be the most common liver disease worldwide. Cardiovascular complications are a leading cause of mortality in NAFLD. Fructose, a common nutrient in the westernized diet, has been reported to be associated with increased cardiovascular risk, but its impact on adolescents with NAFLD is not well understood. We designed a 4-week randomized, controlled, double-blinded beverage intervention study. Twenty-four overweight Hispanic-American adolescents who had hepatic fat >8% on imaging and who were regular consumers of sweet beverages were enrolled and randomized to calorie-matched study-provided fructose only or glucose only beverages. After 4 weeks, there was no significant change in hepatic fat or body weight in either group. In the glucose beverage group there was significantly improved adipose insulin sensitivity, high sensitivity C-reactive protein (hs-CRP), and low-density lipoprotein (LDL) oxidation. These findings demonstrate that reduction of fructose improves several important factors related to cardiovascular disease despite a lack of measurable improvement in hepatic steatosis. Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials.
This one, too:
http://onlinelibrary.wiley.com/doi/10.1002/hep.26299/full
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in adults and children. A number of genetic and environmental factors are known to predispose individuals to NAFLD. Certain dietary sugars, particularly fructose, are suspected to contribute to the development of NAFLD and its progression. The increasing quantity of fructose in the diet comes from sugar additives (most commonly sucrose and high fructose corn syrup) in beverages and processed foods. Substantial links have been demonstrated between increased fructose consumption and obesity, dyslipidemia, and insulin resistance. Growing evidence suggests that fructose contributes to the development and severity of NAFLD. In human studies, fructose is associated with increasing hepatic fat, inflammation, and possibly fibrosis. Whether fructose alone can cause NAFLD or if it serves only as a contributor when consumed excessively in the setting of insulin resistance, positive energy balance, and sedentary lifestyle is unknown. Sufficient evidence exists to support clinical recommendations that fructose intake be limited through decreasing foods and drinks high in added (fructose-containing) sugars. (Hepatology 2013;57:2525–2531)
How many do you want?
First study doesn't support your claim, 2nd one doesn't either unless correlations now = causation, although even the 2nd study's authors don't think that
Do you even science?0 -
I think this abstract sums up the sources of my frustrated confusion on the issue. Note how they know what happens in rats, but humans seem to have different reactions, and they don't know what long term lower sugar consumption is going to do to us even though short term higher consumption does increase intrahepatic fat concentration. But also note that they mention moderate amounts as %10 of energy intake in the US and Europe. In 2010, teens and children were getting %16 of calories from added sugar. (source: http://www.cdc.gov/nchs/data/databriefs/db122.htm). I'm fascinated with the subject, and I want my liver to last a very long time, but there is a lot of contradictory information out there.
Summary
Fructose is mainly consumed with added sugars (sucrose and high fructose corn syrup), and represents up to 10% of total energy intake in the US and in several European countries. This hexose is essentially metabolized in splanchnic tissues, where it is converted into glucose, glycogen, lactate, and, to a minor extent, fatty acids. In animal models, high fructose diets cause the development of obesity, insulin resistance, diabetes mellitus, and dyslipidemia. Ectopic lipid deposition in the liver is an early occurrence upon fructose exposure, and is tightly linked to hepatic insulin resistance. In humans, there is strong evidence, based on several intervention trials, that fructose overfeeding increases fasting and postprandial plasma triglyceride concentrations, which are related to stimulation of hepatic de novo lipogenesis and VLDL-TG secretion, together with decreased VLDL-TG clearance. However, in contrast to animal models, fructose intakes as high as 200 g/day in humans only modestly decreases hepatic insulin sensitivity, and has no effect on no whole body (muscle) insulin sensitivity. A possible explanation may be that insulin resistance and dysglycemia develop mostly in presence of sustained fructose exposures associated with changes in body composition. Such effects are observed with high daily fructose intakes, and there is no solid evidence that fructose, when consumed in moderate amounts, has deleterious effects. There is only limited information regarding the effects of fructose on intrahepatic lipid concentrations. In animal models, high fructose diets clearly stimulate hepatic de novo lipogenesis and cause hepatic steatosis. In addition, some observations suggest that fructose may trigger hepatic inflammation and stimulate the development of hepatic fibrosis. This raises the possibility that fructose may promote the progression of non-alcoholic fatty liver disease to its more severe forms, i.e. non-alcoholic steatohepatitis and cirrhosis. In humans, a short-term fructose overfeeding stimulates de novo lipogenesis and significantly increases intrahepatic fat concentration, without however reaching the proportion encountered in non-alcoholic fatty liver diseases. Whether consumption of lower amounts of fructose over prolonged periods may contribute to the pathogenesis of NAFLD has not been convincingly documented in epidemiological studies and remains to be further assessed.
http://www.sciencedirect.com/science/article/pii/S2210740112001866
LOL "Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). The survey consists of interviews conducted in participants' homes, standardized physical examinations in mobile examination centers (MECs), and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination. Dietary information for this analysis was obtained via an in-person 24-hour dietary recall interview in the MEC."
and lol at your abstract, how many people are consuming over 200g of fructose a day? And animal models? I wonder if DNL occurs at similar rates as humans or it's much much different?
There are other studies, including small scale human ones. I deliberately picked one that is difficult to read (as far as the abstract goes) and contradictory.
But since you don't like that one, let's have a human one:
http://www.mdpi.com/2072-6643/6/8/3187/htm
Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD
Abstract: Nonalcoholic fatty liver disease (NAFLD) is now thought to be the most common liver disease worldwide. Cardiovascular complications are a leading cause of mortality in NAFLD. Fructose, a common nutrient in the westernized diet, has been reported to be associated with increased cardiovascular risk, but its impact on adolescents with NAFLD is not well understood. We designed a 4-week randomized, controlled, double-blinded beverage intervention study. Twenty-four overweight Hispanic-American adolescents who had hepatic fat >8% on imaging and who were regular consumers of sweet beverages were enrolled and randomized to calorie-matched study-provided fructose only or glucose only beverages. After 4 weeks, there was no significant change in hepatic fat or body weight in either group. In the glucose beverage group there was significantly improved adipose insulin sensitivity, high sensitivity C-reactive protein (hs-CRP), and low-density lipoprotein (LDL) oxidation. These findings demonstrate that reduction of fructose improves several important factors related to cardiovascular disease despite a lack of measurable improvement in hepatic steatosis. Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials.
This one, too:
http://onlinelibrary.wiley.com/doi/10.1002/hep.26299/full
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in adults and children. A number of genetic and environmental factors are known to predispose individuals to NAFLD. Certain dietary sugars, particularly fructose, are suspected to contribute to the development of NAFLD and its progression. The increasing quantity of fructose in the diet comes from sugar additives (most commonly sucrose and high fructose corn syrup) in beverages and processed foods. Substantial links have been demonstrated between increased fructose consumption and obesity, dyslipidemia, and insulin resistance. Growing evidence suggests that fructose contributes to the development and severity of NAFLD. In human studies, fructose is associated with increasing hepatic fat, inflammation, and possibly fibrosis. Whether fructose alone can cause NAFLD or if it serves only as a contributor when consumed excessively in the setting of insulin resistance, positive energy balance, and sedentary lifestyle is unknown. Sufficient evidence exists to support clinical recommendations that fructose intake be limited through decreasing foods and drinks high in added (fructose-containing) sugars. (Hepatology 2013;57:2525–2531)
How many do you want?
First study doesn't support your claim, 2nd one doesn't either unless correlations now = causation, although even the 2nd study's authors don't think that
Do you even science?
Like I said, how many do you want? A drop certainly doesn't fill a bucket, but increasingly the studies, however small and not always completely on point, are adding up. And I also said much is unknown and some contradictory (within the same studies, no less!).
By the way, you said earlier no one eats 200g of fructose a day, but I used to down a 2 liter of soda, then go on to have cake, ice cream, and cookies pretty much daily, so if I didn't quite get there, I was damn close. Who knows, I might already have liver damage, meaning the first study could be relevant to me. Quote: "Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials."
Furthermore:
Quote: However, some people develop NAFLD even if they do not have any risk factors. NAFLD affects up to 25% of people in the United States.
Source of second quote: http://www.liverfoundation.org/abouttheliver/info/nafld/0 -
reachingforarainbow wrote: »So while its not always best to eat packaged sweetened yogurt (better to add it yourself, probably have less sugar), its not really that big of a deal. That sugar is looking at natural and added sugar. This is why it should be separated out (into natural and added sugar). It is accounting for lactose, which is a sugar. In regular nonfat, unsweetened milk, in a cup there is 12 grams of sugar... It's really only bad if its added sugar
ahhh yes the evil added sugars....your body does not distinguish between added sugar and natural sugar it is all the same at the molecular level....
Really? My body has no clue when I eat fructose with or without fiber? And it has no clue about the differences between fructose, glucose, and lactose?
If you're right, I'm wasting my time. If you're incorrect, then I should know any differences, too, and food labels should differentiate for us.
are sugar molecules different?
Does the liver treat different sugars differently or not? Does the digestive system act different in any way when we eat high fiber with fructose than when we don't?
so by that logic if I add table sugar to Metamucil it is then bad because added sugar, or is it good because fiber???
Do you actually know the answer? I'd like to hear you actually answer the question without more questions.0 -
I think this abstract sums up the sources of my frustrated confusion on the issue. Note how they know what happens in rats, but humans seem to have different reactions, and they don't know what long term lower sugar consumption is going to do to us even though short term higher consumption does increase intrahepatic fat concentration. But also note that they mention moderate amounts as %10 of energy intake in the US and Europe. In 2010, teens and children were getting %16 of calories from added sugar. (source: http://www.cdc.gov/nchs/data/databriefs/db122.htm). I'm fascinated with the subject, and I want my liver to last a very long time, but there is a lot of contradictory information out there.
Summary
Fructose is mainly consumed with added sugars (sucrose and high fructose corn syrup), and represents up to 10% of total energy intake in the US and in several European countries. This hexose is essentially metabolized in splanchnic tissues, where it is converted into glucose, glycogen, lactate, and, to a minor extent, fatty acids. In animal models, high fructose diets cause the development of obesity, insulin resistance, diabetes mellitus, and dyslipidemia. Ectopic lipid deposition in the liver is an early occurrence upon fructose exposure, and is tightly linked to hepatic insulin resistance. In humans, there is strong evidence, based on several intervention trials, that fructose overfeeding increases fasting and postprandial plasma triglyceride concentrations, which are related to stimulation of hepatic de novo lipogenesis and VLDL-TG secretion, together with decreased VLDL-TG clearance. However, in contrast to animal models, fructose intakes as high as 200 g/day in humans only modestly decreases hepatic insulin sensitivity, and has no effect on no whole body (muscle) insulin sensitivity. A possible explanation may be that insulin resistance and dysglycemia develop mostly in presence of sustained fructose exposures associated with changes in body composition. Such effects are observed with high daily fructose intakes, and there is no solid evidence that fructose, when consumed in moderate amounts, has deleterious effects. There is only limited information regarding the effects of fructose on intrahepatic lipid concentrations. In animal models, high fructose diets clearly stimulate hepatic de novo lipogenesis and cause hepatic steatosis. In addition, some observations suggest that fructose may trigger hepatic inflammation and stimulate the development of hepatic fibrosis. This raises the possibility that fructose may promote the progression of non-alcoholic fatty liver disease to its more severe forms, i.e. non-alcoholic steatohepatitis and cirrhosis. In humans, a short-term fructose overfeeding stimulates de novo lipogenesis and significantly increases intrahepatic fat concentration, without however reaching the proportion encountered in non-alcoholic fatty liver diseases. Whether consumption of lower amounts of fructose over prolonged periods may contribute to the pathogenesis of NAFLD has not been convincingly documented in epidemiological studies and remains to be further assessed.
http://www.sciencedirect.com/science/article/pii/S2210740112001866
LOL "Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). The survey consists of interviews conducted in participants' homes, standardized physical examinations in mobile examination centers (MECs), and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination. Dietary information for this analysis was obtained via an in-person 24-hour dietary recall interview in the MEC."
and lol at your abstract, how many people are consuming over 200g of fructose a day? And animal models? I wonder if DNL occurs at similar rates as humans or it's much much different?
There are other studies, including small scale human ones. I deliberately picked one that is difficult to read (as far as the abstract goes) and contradictory.
But since you don't like that one, let's have a human one:
http://www.mdpi.com/2072-6643/6/8/3187/htm
Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD
Abstract: Nonalcoholic fatty liver disease (NAFLD) is now thought to be the most common liver disease worldwide. Cardiovascular complications are a leading cause of mortality in NAFLD. Fructose, a common nutrient in the westernized diet, has been reported to be associated with increased cardiovascular risk, but its impact on adolescents with NAFLD is not well understood. We designed a 4-week randomized, controlled, double-blinded beverage intervention study. Twenty-four overweight Hispanic-American adolescents who had hepatic fat >8% on imaging and who were regular consumers of sweet beverages were enrolled and randomized to calorie-matched study-provided fructose only or glucose only beverages. After 4 weeks, there was no significant change in hepatic fat or body weight in either group. In the glucose beverage group there was significantly improved adipose insulin sensitivity, high sensitivity C-reactive protein (hs-CRP), and low-density lipoprotein (LDL) oxidation. These findings demonstrate that reduction of fructose improves several important factors related to cardiovascular disease despite a lack of measurable improvement in hepatic steatosis. Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials.
This one, too:
http://onlinelibrary.wiley.com/doi/10.1002/hep.26299/full
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in adults and children. A number of genetic and environmental factors are known to predispose individuals to NAFLD. Certain dietary sugars, particularly fructose, are suspected to contribute to the development of NAFLD and its progression. The increasing quantity of fructose in the diet comes from sugar additives (most commonly sucrose and high fructose corn syrup) in beverages and processed foods. Substantial links have been demonstrated between increased fructose consumption and obesity, dyslipidemia, and insulin resistance. Growing evidence suggests that fructose contributes to the development and severity of NAFLD. In human studies, fructose is associated with increasing hepatic fat, inflammation, and possibly fibrosis. Whether fructose alone can cause NAFLD or if it serves only as a contributor when consumed excessively in the setting of insulin resistance, positive energy balance, and sedentary lifestyle is unknown. Sufficient evidence exists to support clinical recommendations that fructose intake be limited through decreasing foods and drinks high in added (fructose-containing) sugars. (Hepatology 2013;57:2525–2531)
How many do you want?
First study doesn't support your claim, 2nd one doesn't either unless correlations now = causation, although even the 2nd study's authors don't think that
Do you even science?
Like I said, how many do you want? A drop certainly doesn't fill a bucket, but increasingly the studies, however small and not always completely on point, are adding up. And I also said much is unknown and some contradictory (within the same studies, no less!).
By the way, you said earlier no one eats 200g of fructose a day, but I used to down a 2 liter of soda, then go on to have cake, ice cream, and cookies pretty much daily, so if I didn't quite get there, I was damn close. Who knows, I might already have liver damage, meaning the first study could be relevant to me. Quote: "Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials."
Furthermore:
Quote: However, some people develop NAFLD even if they do not have any risk factors. NAFLD affects up to 25% of people in the United States.
Source of second quote: http://www.liverfoundation.org/abouttheliver/info/nafld/
Who said no one eats 200g of fructose again, strawman much?
Oh love the references in that link you provided for that quote, oh wait there are none0 -
I think this abstract sums up the sources of my frustrated confusion on the issue. Note how they know what happens in rats, but humans seem to have different reactions, and they don't know what long term lower sugar consumption is going to do to us even though short term higher consumption does increase intrahepatic fat concentration. But also note that they mention moderate amounts as %10 of energy intake in the US and Europe. In 2010, teens and children were getting %16 of calories from added sugar. (source: http://www.cdc.gov/nchs/data/databriefs/db122.htm). I'm fascinated with the subject, and I want my liver to last a very long time, but there is a lot of contradictory information out there.
Summary
Fructose is mainly consumed with added sugars (sucrose and high fructose corn syrup), and represents up to 10% of total energy intake in the US and in several European countries. This hexose is essentially metabolized in splanchnic tissues, where it is converted into glucose, glycogen, lactate, and, to a minor extent, fatty acids. In animal models, high fructose diets cause the development of obesity, insulin resistance, diabetes mellitus, and dyslipidemia. Ectopic lipid deposition in the liver is an early occurrence upon fructose exposure, and is tightly linked to hepatic insulin resistance. In humans, there is strong evidence, based on several intervention trials, that fructose overfeeding increases fasting and postprandial plasma triglyceride concentrations, which are related to stimulation of hepatic de novo lipogenesis and VLDL-TG secretion, together with decreased VLDL-TG clearance. However, in contrast to animal models, fructose intakes as high as 200 g/day in humans only modestly decreases hepatic insulin sensitivity, and has no effect on no whole body (muscle) insulin sensitivity. A possible explanation may be that insulin resistance and dysglycemia develop mostly in presence of sustained fructose exposures associated with changes in body composition. Such effects are observed with high daily fructose intakes, and there is no solid evidence that fructose, when consumed in moderate amounts, has deleterious effects. There is only limited information regarding the effects of fructose on intrahepatic lipid concentrations. In animal models, high fructose diets clearly stimulate hepatic de novo lipogenesis and cause hepatic steatosis. In addition, some observations suggest that fructose may trigger hepatic inflammation and stimulate the development of hepatic fibrosis. This raises the possibility that fructose may promote the progression of non-alcoholic fatty liver disease to its more severe forms, i.e. non-alcoholic steatohepatitis and cirrhosis. In humans, a short-term fructose overfeeding stimulates de novo lipogenesis and significantly increases intrahepatic fat concentration, without however reaching the proportion encountered in non-alcoholic fatty liver diseases. Whether consumption of lower amounts of fructose over prolonged periods may contribute to the pathogenesis of NAFLD has not been convincingly documented in epidemiological studies and remains to be further assessed.
http://www.sciencedirect.com/science/article/pii/S2210740112001866
LOL "Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). The survey consists of interviews conducted in participants' homes, standardized physical examinations in mobile examination centers (MECs), and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination. Dietary information for this analysis was obtained via an in-person 24-hour dietary recall interview in the MEC."
and lol at your abstract, how many people are consuming over 200g of fructose a day? And animal models? I wonder if DNL occurs at similar rates as humans or it's much much different?
There are other studies, including small scale human ones. I deliberately picked one that is difficult to read (as far as the abstract goes) and contradictory.
But since you don't like that one, let's have a human one:
http://www.mdpi.com/2072-6643/6/8/3187/htm
Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD
Abstract: Nonalcoholic fatty liver disease (NAFLD) is now thought to be the most common liver disease worldwide. Cardiovascular complications are a leading cause of mortality in NAFLD. Fructose, a common nutrient in the westernized diet, has been reported to be associated with increased cardiovascular risk, but its impact on adolescents with NAFLD is not well understood. We designed a 4-week randomized, controlled, double-blinded beverage intervention study. Twenty-four overweight Hispanic-American adolescents who had hepatic fat >8% on imaging and who were regular consumers of sweet beverages were enrolled and randomized to calorie-matched study-provided fructose only or glucose only beverages. After 4 weeks, there was no significant change in hepatic fat or body weight in either group. In the glucose beverage group there was significantly improved adipose insulin sensitivity, high sensitivity C-reactive protein (hs-CRP), and low-density lipoprotein (LDL) oxidation. These findings demonstrate that reduction of fructose improves several important factors related to cardiovascular disease despite a lack of measurable improvement in hepatic steatosis. Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials.
This one, too:
http://onlinelibrary.wiley.com/doi/10.1002/hep.26299/full
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in adults and children. A number of genetic and environmental factors are known to predispose individuals to NAFLD. Certain dietary sugars, particularly fructose, are suspected to contribute to the development of NAFLD and its progression. The increasing quantity of fructose in the diet comes from sugar additives (most commonly sucrose and high fructose corn syrup) in beverages and processed foods. Substantial links have been demonstrated between increased fructose consumption and obesity, dyslipidemia, and insulin resistance. Growing evidence suggests that fructose contributes to the development and severity of NAFLD. In human studies, fructose is associated with increasing hepatic fat, inflammation, and possibly fibrosis. Whether fructose alone can cause NAFLD or if it serves only as a contributor when consumed excessively in the setting of insulin resistance, positive energy balance, and sedentary lifestyle is unknown. Sufficient evidence exists to support clinical recommendations that fructose intake be limited through decreasing foods and drinks high in added (fructose-containing) sugars. (Hepatology 2013;57:2525–2531)
How many do you want?
First study doesn't support your claim, 2nd one doesn't either unless correlations now = causation, although even the 2nd study's authors don't think that
Do you even science?
Like I said, how many do you want? A drop certainly doesn't fill a bucket, but increasingly the studies, however small and not always completely on point, are adding up. And I also said much is unknown and some contradictory (within the same studies, no less!).
By the way, you said earlier no one eats 200g of fructose a day, but I used to down a 2 liter of soda, then go on to have cake, ice cream, and cookies pretty much daily, so if I didn't quite get there, I was damn close. Who knows, I might already have liver damage, meaning the first study could be relevant to me. Quote: "Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials."
Furthermore:
Quote: However, some people develop NAFLD even if they do not have any risk factors. NAFLD affects up to 25% of people in the United States.
Source of second quote: http://www.liverfoundation.org/abouttheliver/info/nafld/
Who said no one eats 200g of fructose again, strawman much?
Oh love the references in that link you provided for that quote, oh wait there are none
You're right, you said 'how many' not no one. Well, I was one. And yes, I'm concerned about the possibility that my liver is fat because of that, or genetic factors, or both, based on what I've been reading and doing my best to learn.0 -
reachingforarainbow wrote: »So while its not always best to eat packaged sweetened yogurt (better to add it yourself, probably have less sugar), its not really that big of a deal. That sugar is looking at natural and added sugar. This is why it should be separated out (into natural and added sugar). It is accounting for lactose, which is a sugar. In regular nonfat, unsweetened milk, in a cup there is 12 grams of sugar... It's really only bad if its added sugar
ahhh yes the evil added sugars....your body does not distinguish between added sugar and natural sugar it is all the same at the molecular level....
Really? My body has no clue when I eat fructose with or without fiber? And it has no clue about the differences between fructose, glucose, and lactose?
If you're right, I'm wasting my time. If you're incorrect, then I should know any differences, too, and food labels should differentiate for us.
are sugar molecules different?
Does the liver treat different sugars differently or not? Does the digestive system act different in any way when we eat high fiber with fructose than when we don't?
so by that logic if I add table sugar to Metamucil it is then bad because added sugar, or is it good because fiber???
Do you actually know the answer? I'd like to hear you actually answer the question without more questions.
the answer to what..?0 -
You're right, there is something wrong with that breakfast. But it's not the sugar content, it's that a container of yogurt isn't a meal, it's a snack.0
-
kcmccormack wrote: »You can make alot of your own "healthier" versions of granola bars or cookies by using fruit purees or vegetable purees in your baking and staying away from honeys, agave or other sweeteners instead of placing your faith in whatever snack some huge corporation MARKETED as "healthy" that's packed with garbage like high fructose corn syrup, refined sugars or whatever else they put in there. You can satisfy your sweet tooth without buying stuff that's sweetened to the nth degree for you.
I just found out I'm diabetic. I have to relearn how to choose foods now. Man, this blows. I need to find out which fruits and vegetables are still okay and which I need to ditch.
Man, this blows. I need to find out which fruits and vegetables are still okay and which I need to ditch.
I would suggest going to bloodsugar101.com. They have a plan that helps you figure out which foods are better for YOU specifically and which ones to steer clear of. There is a ton of really good info on there. What I have found is limiting fruit to berries or special occasions for things like bananas and apples. Grapes are higher in sugar than berries but with grapes its easier to limit your portions than with an apple. For veggies, its usually things like potatoes and corn, and anything with "sweet" in the name. I've eliminated corn, cut way, way back on potatoes, and limit sweet potatoes to special occasion for now. But again, try to get a plan that affects your limits and you'll have a better grasp of things long term. What affects me may not affect you the same way. Also, you might want to visit the Low Carbers group here, if you haven't already. Lots of good ideas and recipe sights.0 -
I think this abstract sums up the sources of my frustrated confusion on the issue. Note how they know what happens in rats, but humans seem to have different reactions, and they don't know what long term lower sugar consumption is going to do to us even though short term higher consumption does increase intrahepatic fat concentration. But also note that they mention moderate amounts as %10 of energy intake in the US and Europe. In 2010, teens and children were getting %16 of calories from added sugar. (source: http://www.cdc.gov/nchs/data/databriefs/db122.htm). I'm fascinated with the subject, and I want my liver to last a very long time, but there is a lot of contradictory information out there.
Summary
Fructose is mainly consumed with added sugars (sucrose and high fructose corn syrup), and represents up to 10% of total energy intake in the US and in several European countries. This hexose is essentially metabolized in splanchnic tissues, where it is converted into glucose, glycogen, lactate, and, to a minor extent, fatty acids. In animal models, high fructose diets cause the development of obesity, insulin resistance, diabetes mellitus, and dyslipidemia. Ectopic lipid deposition in the liver is an early occurrence upon fructose exposure, and is tightly linked to hepatic insulin resistance. In humans, there is strong evidence, based on several intervention trials, that fructose overfeeding increases fasting and postprandial plasma triglyceride concentrations, which are related to stimulation of hepatic de novo lipogenesis and VLDL-TG secretion, together with decreased VLDL-TG clearance. However, in contrast to animal models, fructose intakes as high as 200 g/day in humans only modestly decreases hepatic insulin sensitivity, and has no effect on no whole body (muscle) insulin sensitivity. A possible explanation may be that insulin resistance and dysglycemia develop mostly in presence of sustained fructose exposures associated with changes in body composition. Such effects are observed with high daily fructose intakes, and there is no solid evidence that fructose, when consumed in moderate amounts, has deleterious effects. There is only limited information regarding the effects of fructose on intrahepatic lipid concentrations. In animal models, high fructose diets clearly stimulate hepatic de novo lipogenesis and cause hepatic steatosis. In addition, some observations suggest that fructose may trigger hepatic inflammation and stimulate the development of hepatic fibrosis. This raises the possibility that fructose may promote the progression of non-alcoholic fatty liver disease to its more severe forms, i.e. non-alcoholic steatohepatitis and cirrhosis. In humans, a short-term fructose overfeeding stimulates de novo lipogenesis and significantly increases intrahepatic fat concentration, without however reaching the proportion encountered in non-alcoholic fatty liver diseases. Whether consumption of lower amounts of fructose over prolonged periods may contribute to the pathogenesis of NAFLD has not been convincingly documented in epidemiological studies and remains to be further assessed.
http://www.sciencedirect.com/science/article/pii/S2210740112001866
LOL "Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). The survey consists of interviews conducted in participants' homes, standardized physical examinations in mobile examination centers (MECs), and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination. Dietary information for this analysis was obtained via an in-person 24-hour dietary recall interview in the MEC."
and lol at your abstract, how many people are consuming over 200g of fructose a day? And animal models? I wonder if DNL occurs at similar rates as humans or it's much much different?
There are other studies, including small scale human ones. I deliberately picked one that is difficult to read (as far as the abstract goes) and contradictory.
But since you don't like that one, let's have a human one:
http://www.mdpi.com/2072-6643/6/8/3187/htm
Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD
Abstract: Nonalcoholic fatty liver disease (NAFLD) is now thought to be the most common liver disease worldwide. Cardiovascular complications are a leading cause of mortality in NAFLD. Fructose, a common nutrient in the westernized diet, has been reported to be associated with increased cardiovascular risk, but its impact on adolescents with NAFLD is not well understood. We designed a 4-week randomized, controlled, double-blinded beverage intervention study. Twenty-four overweight Hispanic-American adolescents who had hepatic fat >8% on imaging and who were regular consumers of sweet beverages were enrolled and randomized to calorie-matched study-provided fructose only or glucose only beverages. After 4 weeks, there was no significant change in hepatic fat or body weight in either group. In the glucose beverage group there was significantly improved adipose insulin sensitivity, high sensitivity C-reactive protein (hs-CRP), and low-density lipoprotein (LDL) oxidation. These findings demonstrate that reduction of fructose improves several important factors related to cardiovascular disease despite a lack of measurable improvement in hepatic steatosis. Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials.
This one, too:
http://onlinelibrary.wiley.com/doi/10.1002/hep.26299/full
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in adults and children. A number of genetic and environmental factors are known to predispose individuals to NAFLD. Certain dietary sugars, particularly fructose, are suspected to contribute to the development of NAFLD and its progression. The increasing quantity of fructose in the diet comes from sugar additives (most commonly sucrose and high fructose corn syrup) in beverages and processed foods. Substantial links have been demonstrated between increased fructose consumption and obesity, dyslipidemia, and insulin resistance. Growing evidence suggests that fructose contributes to the development and severity of NAFLD. In human studies, fructose is associated with increasing hepatic fat, inflammation, and possibly fibrosis. Whether fructose alone can cause NAFLD or if it serves only as a contributor when consumed excessively in the setting of insulin resistance, positive energy balance, and sedentary lifestyle is unknown. Sufficient evidence exists to support clinical recommendations that fructose intake be limited through decreasing foods and drinks high in added (fructose-containing) sugars. (Hepatology 2013;57:2525–2531)
How many do you want?
First study doesn't support your claim, 2nd one doesn't either unless correlations now = causation, although even the 2nd study's authors don't think that
Do you even science?
Like I said, how many do you want? A drop certainly doesn't fill a bucket, but increasingly the studies, however small and not always completely on point, are adding up. And I also said much is unknown and some contradictory (within the same studies, no less!).
By the way, you said earlier no one eats 200g of fructose a day, but I used to down a 2 liter of soda, then go on to have cake, ice cream, and cookies pretty much daily, so if I didn't quite get there, I was damn close. Who knows, I might already have liver damage, meaning the first study could be relevant to me. Quote: "Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials."
Furthermore:
Quote: However, some people develop NAFLD even if they do not have any risk factors. NAFLD affects up to 25% of people in the United States.
Source of second quote: http://www.liverfoundation.org/abouttheliver/info/nafld/
Who said no one eats 200g of fructose again, strawman much?
Oh love the references in that link you provided for that quote, oh wait there are none
You're right, you said 'how many' not no one. Well, I was one. And yes, I'm concerned about the possibility that my liver is fat because of that, or genetic factors, or both, based on what I've been reading and doing my best to learn.
So now you are someone that consumed 200g of fructose a day but before you said you're not sure. At least you're being consistent
0 -
the old sugar dilemma , sugars and fats , they are all NOT the same you will need to see the GI index for the type of sugar you consume some will increase your insulin more than others. i know there are people who do not believe in the system but i do0
-
Am I mistaken, or did some people write that they think refined sugar is good for you??
People sure fight awfully hard when someone says they want to eliminate sugar, though. I know the majority are saying its fine in moderation so long as there is no medical issue but some people seem to come out swinging whenever the topic is introduced. What never really makes sense to me, though, is WHY they're fighting so hard. If someone eliminates a lot of unnecessary sugar, which I take to mean things like candy and cake (not fruit, seriously who thinks people are really talking about fruit?), then they are most likely eating at a deficit, therefore losing weight. Why is it seen as such a horrible thing if someone wants to cut back on it?0 -
reachingforarainbow wrote: »So while its not always best to eat packaged sweetened yogurt (better to add it yourself, probably have less sugar), its not really that big of a deal. That sugar is looking at natural and added sugar. This is why it should be separated out (into natural and added sugar). It is accounting for lactose, which is a sugar. In regular nonfat, unsweetened milk, in a cup there is 12 grams of sugar... It's really only bad if its added sugar
ahhh yes the evil added sugars....your body does not distinguish between added sugar and natural sugar it is all the same at the molecular level....
Really? My body has no clue when I eat fructose with or without fiber? And it has no clue about the differences between fructose, glucose, and lactose?
If you're right, I'm wasting my time. If you're incorrect, then I should know any differences, too, and food labels should differentiate for us.
are sugar molecules different?
Does the liver treat different sugars differently or not? Does the digestive system act different in any way when we eat high fiber with fructose than when we don't?
so by that logic if I add table sugar to Metamucil it is then bad because added sugar, or is it good because fiber???
Do you actually know the answer? I'd like to hear you actually answer the question without more questions.
the answer to what..?
The part I quoted. Nevermind, you don't, I can see that. That's okay.0 -
Am I mistaken, or did some people write that they think refined sugar is good for you??
People sure fight awfully hard when someone says they want to eliminate sugar, though. I know the majority are saying its fine in moderation so long as there is no medical issue but some people seem to come out swinging whenever the topic is introduced. What never really makes sense to me, though, is WHY they're fighting so hard. If someone eliminates a lot of unnecessary sugar, which I take to mean things like candy and cake (not fruit, seriously who thinks people are really talking about fruit?), then they are most likely eating at a deficit, therefore losing weight. Why is it seen as such a horrible thing if someone wants to cut back on it?
The OP seems to feel completely defeated and failing, and associating those feelings with food just because someone told her what is and is not healthy is completely unnecessary.0 -
This was a bit of honey in greek yogurt. Not anywhere near an OD on sugar. Like a few others here I was more concerned with paucity of this breakfast.
http://www.caloriecount.com/calories-greek-gods-traditional-honey-yogurt-i1268220 -
I think this abstract sums up the sources of my frustrated confusion on the issue. Note how they know what happens in rats, but humans seem to have different reactions, and they don't know what long term lower sugar consumption is going to do to us even though short term higher consumption does increase intrahepatic fat concentration. But also note that they mention moderate amounts as %10 of energy intake in the US and Europe. In 2010, teens and children were getting %16 of calories from added sugar. (source: http://www.cdc.gov/nchs/data/databriefs/db122.htm). I'm fascinated with the subject, and I want my liver to last a very long time, but there is a lot of contradictory information out there.
Summary
Fructose is mainly consumed with added sugars (sucrose and high fructose corn syrup), and represents up to 10% of total energy intake in the US and in several European countries. This hexose is essentially metabolized in splanchnic tissues, where it is converted into glucose, glycogen, lactate, and, to a minor extent, fatty acids. In animal models, high fructose diets cause the development of obesity, insulin resistance, diabetes mellitus, and dyslipidemia. Ectopic lipid deposition in the liver is an early occurrence upon fructose exposure, and is tightly linked to hepatic insulin resistance. In humans, there is strong evidence, based on several intervention trials, that fructose overfeeding increases fasting and postprandial plasma triglyceride concentrations, which are related to stimulation of hepatic de novo lipogenesis and VLDL-TG secretion, together with decreased VLDL-TG clearance. However, in contrast to animal models, fructose intakes as high as 200 g/day in humans only modestly decreases hepatic insulin sensitivity, and has no effect on no whole body (muscle) insulin sensitivity. A possible explanation may be that insulin resistance and dysglycemia develop mostly in presence of sustained fructose exposures associated with changes in body composition. Such effects are observed with high daily fructose intakes, and there is no solid evidence that fructose, when consumed in moderate amounts, has deleterious effects. There is only limited information regarding the effects of fructose on intrahepatic lipid concentrations. In animal models, high fructose diets clearly stimulate hepatic de novo lipogenesis and cause hepatic steatosis. In addition, some observations suggest that fructose may trigger hepatic inflammation and stimulate the development of hepatic fibrosis. This raises the possibility that fructose may promote the progression of non-alcoholic fatty liver disease to its more severe forms, i.e. non-alcoholic steatohepatitis and cirrhosis. In humans, a short-term fructose overfeeding stimulates de novo lipogenesis and significantly increases intrahepatic fat concentration, without however reaching the proportion encountered in non-alcoholic fatty liver diseases. Whether consumption of lower amounts of fructose over prolonged periods may contribute to the pathogenesis of NAFLD has not been convincingly documented in epidemiological studies and remains to be further assessed.
http://www.sciencedirect.com/science/article/pii/S2210740112001866
LOL "Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). The survey consists of interviews conducted in participants' homes, standardized physical examinations in mobile examination centers (MECs), and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination. Dietary information for this analysis was obtained via an in-person 24-hour dietary recall interview in the MEC."
and lol at your abstract, how many people are consuming over 200g of fructose a day? And animal models? I wonder if DNL occurs at similar rates as humans or it's much much different?
There are other studies, including small scale human ones. I deliberately picked one that is difficult to read (as far as the abstract goes) and contradictory.
But since you don't like that one, let's have a human one:
http://www.mdpi.com/2072-6643/6/8/3187/htm
Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD
Abstract: Nonalcoholic fatty liver disease (NAFLD) is now thought to be the most common liver disease worldwide. Cardiovascular complications are a leading cause of mortality in NAFLD. Fructose, a common nutrient in the westernized diet, has been reported to be associated with increased cardiovascular risk, but its impact on adolescents with NAFLD is not well understood. We designed a 4-week randomized, controlled, double-blinded beverage intervention study. Twenty-four overweight Hispanic-American adolescents who had hepatic fat >8% on imaging and who were regular consumers of sweet beverages were enrolled and randomized to calorie-matched study-provided fructose only or glucose only beverages. After 4 weeks, there was no significant change in hepatic fat or body weight in either group. In the glucose beverage group there was significantly improved adipose insulin sensitivity, high sensitivity C-reactive protein (hs-CRP), and low-density lipoprotein (LDL) oxidation. These findings demonstrate that reduction of fructose improves several important factors related to cardiovascular disease despite a lack of measurable improvement in hepatic steatosis. Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials.
This one, too:
http://onlinelibrary.wiley.com/doi/10.1002/hep.26299/full
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in adults and children. A number of genetic and environmental factors are known to predispose individuals to NAFLD. Certain dietary sugars, particularly fructose, are suspected to contribute to the development of NAFLD and its progression. The increasing quantity of fructose in the diet comes from sugar additives (most commonly sucrose and high fructose corn syrup) in beverages and processed foods. Substantial links have been demonstrated between increased fructose consumption and obesity, dyslipidemia, and insulin resistance. Growing evidence suggests that fructose contributes to the development and severity of NAFLD. In human studies, fructose is associated with increasing hepatic fat, inflammation, and possibly fibrosis. Whether fructose alone can cause NAFLD or if it serves only as a contributor when consumed excessively in the setting of insulin resistance, positive energy balance, and sedentary lifestyle is unknown. Sufficient evidence exists to support clinical recommendations that fructose intake be limited through decreasing foods and drinks high in added (fructose-containing) sugars. (Hepatology 2013;57:2525–2531)
How many do you want?
First study doesn't support your claim, 2nd one doesn't either unless correlations now = causation, although even the 2nd study's authors don't think that
Do you even science?
Like I said, how many do you want? A drop certainly doesn't fill a bucket, but increasingly the studies, however small and not always completely on point, are adding up. And I also said much is unknown and some contradictory (within the same studies, no less!).
By the way, you said earlier no one eats 200g of fructose a day, but I used to down a 2 liter of soda, then go on to have cake, ice cream, and cookies pretty much daily, so if I didn't quite get there, I was damn close. Who knows, I might already have liver damage, meaning the first study could be relevant to me. Quote: "Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials."
Furthermore:
Quote: However, some people develop NAFLD even if they do not have any risk factors. NAFLD affects up to 25% of people in the United States.
Source of second quote: http://www.liverfoundation.org/abouttheliver/info/nafld/
Who said no one eats 200g of fructose again, strawman much?
Oh love the references in that link you provided for that quote, oh wait there are none
You're right, you said 'how many' not no one. Well, I was one. And yes, I'm concerned about the possibility that my liver is fat because of that, or genetic factors, or both, based on what I've been reading and doing my best to learn.
So now you are someone that consumed 200g of fructose a day but before you said you're not sure. At least you're being consistent
I looked up grams of sugar in a 2 liter of soda this morning. It's over 200g of sugar. But it's not all fructose, correct? It's a mix. %55 percent is fructose. So halve that, meaning over 100 grams of it was fructose. Then add in the cake, ice cream, and cookies, and I was almost certainly over 200 almost every day for the two years I was eating like an idiot. Yeah, I have reason to think I could have done some damage. And my diet wasn't that great before that, either!0 -
The life of a diabetic is one of balance. There are no bad foods or fruits. If you get more than one macro in a meal and pick calorie-dense fiber-rich foods more often, your blood sugars will be more stable. First two rules; time your meals starting with breakfast the same time every day. No more than 2 1/2 hours between each meal or snack (except for sleeping). Second, balance your plate and snack to incorporate your macros. The plate method is easy to remember.I just found out I'm diabetic. I have to relearn how to choose foods now. Man, this blows. I need to find out which fruits and vegetables are still okay and which I need to ditch.
0 -
fructose and high fructose corn syrup are 2 totally different things0
-
I made a table of sugars the other day, considering this topic comes up at least twice a day.
So ironic that honey ("natural", therefore "good" to the back-to-nature crowd) is 41% fructose, whereas high fructose corn syrup ("man-made", therefore responsible for all evils to the back-to-nature crowd) is 55% fructose. The remainder for both is mainly glucose. So is fructose "good" or "bad"? Neither, hahahahaha.
Chemically, there are differences. Fructose:
Glucose: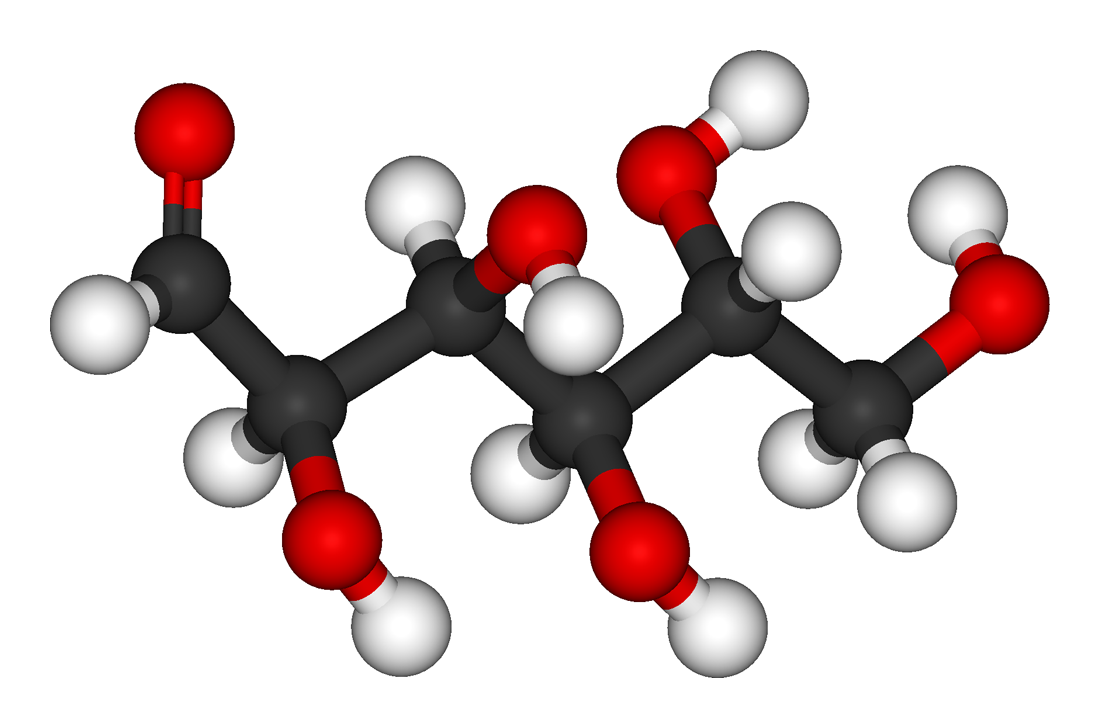
Confused? Our bodies aren't. We matabolise them all.
You are my hero! lol.
0 -
I think this abstract sums up the sources of my frustrated confusion on the issue. Note how they know what happens in rats, but humans seem to have different reactions, and they don't know what long term lower sugar consumption is going to do to us even though short term higher consumption does increase intrahepatic fat concentration. But also note that they mention moderate amounts as %10 of energy intake in the US and Europe. In 2010, teens and children were getting %16 of calories from added sugar. (source: http://www.cdc.gov/nchs/data/databriefs/db122.htm). I'm fascinated with the subject, and I want my liver to last a very long time, but there is a lot of contradictory information out there.
Summary
Fructose is mainly consumed with added sugars (sucrose and high fructose corn syrup), and represents up to 10% of total energy intake in the US and in several European countries. This hexose is essentially metabolized in splanchnic tissues, where it is converted into glucose, glycogen, lactate, and, to a minor extent, fatty acids. In animal models, high fructose diets cause the development of obesity, insulin resistance, diabetes mellitus, and dyslipidemia. Ectopic lipid deposition in the liver is an early occurrence upon fructose exposure, and is tightly linked to hepatic insulin resistance. In humans, there is strong evidence, based on several intervention trials, that fructose overfeeding increases fasting and postprandial plasma triglyceride concentrations, which are related to stimulation of hepatic de novo lipogenesis and VLDL-TG secretion, together with decreased VLDL-TG clearance. However, in contrast to animal models, fructose intakes as high as 200 g/day in humans only modestly decreases hepatic insulin sensitivity, and has no effect on no whole body (muscle) insulin sensitivity. A possible explanation may be that insulin resistance and dysglycemia develop mostly in presence of sustained fructose exposures associated with changes in body composition. Such effects are observed with high daily fructose intakes, and there is no solid evidence that fructose, when consumed in moderate amounts, has deleterious effects. There is only limited information regarding the effects of fructose on intrahepatic lipid concentrations. In animal models, high fructose diets clearly stimulate hepatic de novo lipogenesis and cause hepatic steatosis. In addition, some observations suggest that fructose may trigger hepatic inflammation and stimulate the development of hepatic fibrosis. This raises the possibility that fructose may promote the progression of non-alcoholic fatty liver disease to its more severe forms, i.e. non-alcoholic steatohepatitis and cirrhosis. In humans, a short-term fructose overfeeding stimulates de novo lipogenesis and significantly increases intrahepatic fat concentration, without however reaching the proportion encountered in non-alcoholic fatty liver diseases. Whether consumption of lower amounts of fructose over prolonged periods may contribute to the pathogenesis of NAFLD has not been convincingly documented in epidemiological studies and remains to be further assessed.
http://www.sciencedirect.com/science/article/pii/S2210740112001866
LOL "Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). The survey consists of interviews conducted in participants' homes, standardized physical examinations in mobile examination centers (MECs), and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination. Dietary information for this analysis was obtained via an in-person 24-hour dietary recall interview in the MEC."
and lol at your abstract, how many people are consuming over 200g of fructose a day? And animal models? I wonder if DNL occurs at similar rates as humans or it's much much different?
There are other studies, including small scale human ones. I deliberately picked one that is difficult to read (as far as the abstract goes) and contradictory.
But since you don't like that one, let's have a human one:
http://www.mdpi.com/2072-6643/6/8/3187/htm
Dietary Fructose Reduction Improves Markers of Cardiovascular Disease Risk in Hispanic-American Adolescents with NAFLD
Abstract: Nonalcoholic fatty liver disease (NAFLD) is now thought to be the most common liver disease worldwide. Cardiovascular complications are a leading cause of mortality in NAFLD. Fructose, a common nutrient in the westernized diet, has been reported to be associated with increased cardiovascular risk, but its impact on adolescents with NAFLD is not well understood. We designed a 4-week randomized, controlled, double-blinded beverage intervention study. Twenty-four overweight Hispanic-American adolescents who had hepatic fat >8% on imaging and who were regular consumers of sweet beverages were enrolled and randomized to calorie-matched study-provided fructose only or glucose only beverages. After 4 weeks, there was no significant change in hepatic fat or body weight in either group. In the glucose beverage group there was significantly improved adipose insulin sensitivity, high sensitivity C-reactive protein (hs-CRP), and low-density lipoprotein (LDL) oxidation. These findings demonstrate that reduction of fructose improves several important factors related to cardiovascular disease despite a lack of measurable improvement in hepatic steatosis. Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials.
This one, too:
http://onlinelibrary.wiley.com/doi/10.1002/hep.26299/full
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease in adults and children. A number of genetic and environmental factors are known to predispose individuals to NAFLD. Certain dietary sugars, particularly fructose, are suspected to contribute to the development of NAFLD and its progression. The increasing quantity of fructose in the diet comes from sugar additives (most commonly sucrose and high fructose corn syrup) in beverages and processed foods. Substantial links have been demonstrated between increased fructose consumption and obesity, dyslipidemia, and insulin resistance. Growing evidence suggests that fructose contributes to the development and severity of NAFLD. In human studies, fructose is associated with increasing hepatic fat, inflammation, and possibly fibrosis. Whether fructose alone can cause NAFLD or if it serves only as a contributor when consumed excessively in the setting of insulin resistance, positive energy balance, and sedentary lifestyle is unknown. Sufficient evidence exists to support clinical recommendations that fructose intake be limited through decreasing foods and drinks high in added (fructose-containing) sugars. (Hepatology 2013;57:2525–2531)
How many do you want?
First study doesn't support your claim, 2nd one doesn't either unless correlations now = causation, although even the 2nd study's authors don't think that
Do you even science?
Like I said, how many do you want? A drop certainly doesn't fill a bucket, but increasingly the studies, however small and not always completely on point, are adding up. And I also said much is unknown and some contradictory (within the same studies, no less!).
By the way, you said earlier no one eats 200g of fructose a day, but I used to down a 2 liter of soda, then go on to have cake, ice cream, and cookies pretty much daily, so if I didn't quite get there, I was damn close. Who knows, I might already have liver damage, meaning the first study could be relevant to me. Quote: "Reducing dietary fructose may be an effective intervention to blunt atherosclerosis progression among NAFLD patients and should be evaluated in longer term clinical trials."
Furthermore:
Quote: However, some people develop NAFLD even if they do not have any risk factors. NAFLD affects up to 25% of people in the United States.
Source of second quote: http://www.liverfoundation.org/abouttheliver/info/nafld/
Who said no one eats 200g of fructose again, strawman much?
Oh love the references in that link you provided for that quote, oh wait there are none
You're right, you said 'how many' not no one. Well, I was one. And yes, I'm concerned about the possibility that my liver is fat because of that, or genetic factors, or both, based on what I've been reading and doing my best to learn.
So now you are someone that consumed 200g of fructose a day but before you said you're not sure. At least you're being consistent
I looked up grams of sugar in a 2 liter of soda this morning. But it's not all fructose, correct? It's a mix. %55 percent is fructose. So halve that, meaning over 100 grams of it was fructose. Then add in the cake, ice cream, and cookies, and I was almost certainly over 200 every day for the two years I was eating like an idiot. Yeah, I have reason to think I could have done some damage.
You'd need to have had roughly 166g of "sugar" in addition to the 2 liter to hit approx 200g of fructose a day. Perhaps you were consuming that much and certainly others do too, but what % do you think consumes that amount? If it's a small % then how realistic was the researcher for using that amount?0 -
Bootcamp, high fructose corn syrup is made up of fructose and glucose.0
-
Am I mistaken, or did some people write that they think refined sugar is good for you??
People sure fight awfully hard when someone says they want to eliminate sugar, though. I know the majority are saying its fine in moderation so long as there is no medical issue but some people seem to come out swinging whenever the topic is introduced. What never really makes sense to me, though, is WHY they're fighting so hard. If someone eliminates a lot of unnecessary sugar, which I take to mean things like candy and cake (not fruit, seriously who thinks people are really talking about fruit?), then they are most likely eating at a deficit, therefore losing weight. Why is it seen as such a horrible thing if someone wants to cut back on it?
The OP seems to feel completely defeated and failing, and associating those feelings with food just because someone told her what is and is not healthy is completely unnecessary.
I guess it read differently to me. I thought it was just shock and frustration. I've been there and done that and I suppose there was a small feeling of defeat but I just read the labels a little closer next time. But if she's posted something else, I've missed it so you may be right.0 -
The life of a diabetic is one of balance. There are no bad foods or fruits. If you get more than one macro in a meal and pick calorie-dense fiber-rich foods more often, your blood sugars will be more stable. First two rules; time your meals starting with breakfast the same time every day. No more than 2 1/2 hours between each meal or snack (except for sleeping). Second, balance your plate and snack to incorporate your macros. The plate method is easy to remember.I just found out I'm diabetic. I have to relearn how to choose foods now. Man, this blows. I need to find out which fruits and vegetables are still okay and which I need to ditch.
There are no "bad" foods at first, perhaps. But the longer you have diabetes the harder it can be to process certain things. At least that's what I'm currently finding out.0













This discussion has been closed.
Categories
- All Categories
- 1.4M Health, Wellness and Goals
- 398.2K Introduce Yourself
- 44.7K Getting Started
- 261K Health and Weight Loss
- 176.4K Food and Nutrition
- 47.7K Recipes
- 233K Fitness and Exercise
- 462 Sleep, Mindfulness and Overall Wellness
- 6.5K Goal: Maintaining Weight
- 8.7K Goal: Gaining Weight and Body Building
- 153.5K Motivation and Support
- 8.4K Challenges
- 1.4K Debate Club
- 96.5K Chit-Chat
- 2.6K Fun and Games
- 4.8K MyFitnessPal Information
- 12 News and Announcements
- 21 MyFitnessPal Academy
- 1.6K Feature Suggestions and Ideas
- 3.2K MyFitnessPal Tech Support Questions