Ketogenic Diet
Replies
-
Nice going! Still not sure if it's feasible. Quite probably you already had that muscle and saw it when you leaned up.
What all did you do? Any use of chemicals?
Well I can certainly assure you it was not there at the start and definitely no use of 'chemicals'. I lost 40lbs doing a mix of FB and HIIT sessions, ate a high protein and clean diet and to a calorie deficit of 1800 cals a day, only supplements I took was protein shakes, fish oils and multivitamins. Also, in terms of strength gains, these were huge. At my peak I was squatting 145kg for 3 reps ( I only weighed 72kg at the time) was able to do 21 chins and bench press was 110kg for my one rep max. I also did 86 press ups in 60 seconds where at the start I was able to do around 40ish. So yes, it is possible to build muscle while on a calorie deficit! But that was because I was chunky to start with... Once I got lean then yes, my progress would have stalled and I would have had to eat more to build more muscle. But, if you are looking to lose weight then you can but fat and build muscle at the same time.
you did exactly what i've been telling this guy to do. love it! great work man!0 -
that's interesting and i'll look into it, but what does it have to do with how many calories you burn daily, and thus, your TDEE? how much are you exercising?
If MHR formula=wrong
Maybe TDEE multiplier formula = wrong
EDIT: You outright dismissed the possibility that the MHR is wrong and that I was at fault. Then I linked an article that suggests MHR formula is wrong, and now you realize there's validity in what I said. Think about that.0 -
that's interesting and i'll look into it, but what does it have to do with how many calories you burn daily, and thus, your TDEE? how much are you exercising?
If MHR formula=wrong
Maybe TDEE multiplier formula = wrong
EDIT: You outright dismissed the possibility that the MHR is wrong and that I was at fault. Then I linked an article that suggests MHR formula is wrong, and now you realize there's validity in what I said. Think about that.
that's a huge unfounded jump from MHR to TDEE, also that article is over 10 years old. can you find something newer? why hasn't it taken hold if it were accurate? I'm not saying it isn't true, but to say that max heart rates are a tad off means your daily heart rate or calorie burn is off just... doesn't make any sense0 -
**** it man, do what you want. not one person has come to your defense, and that's saying something given that I'm the one arguing with you. if I were miles off base, there would be a dozen people in here trying to stick it to me, but even folks I typically disagree with are agreeing with me here.
but cover your ears and eyes and ignore science and try it your way. i wish you luck.0 -
I find that my heart rate gets much higher at lower intensities when I either have not been eating enough or am on the second or third workout of the day.
I noticed that yesterday, I was in full on keto flu and my heart rate skyrocketed compared to normal. Finally hit 180 when I never could before.0 -
YEAH BEEN THERE DONE THAT EASILY ONE OF THE WORST UNHEALTHIEST AND INEFFECTIVE DIETS EVER.....I STRONGLY SUGGEST THE EXACT OPPOSITE! ITS FRIDAYYYYY:)
KRISTIAN ROCCO0 -
Bump. I'd like to read this later.0
-
Because as previously stated, gaining muscle on a cut is not feasible.
Oh and...
Fat does not "convert to muscle".why not use the mass you already have and just convert it to muscle...?
no obviously it doesn't actually convert, it's just a turn of phrase.
but if your body has other fuel sources to burn besides your muscle tissue, it will burn them, thus shedding fat at the same time as your lifting heavy builds muscle size and strength
Your body doesn't work like that. Burning fat is a catabolic process, gaining muscle is an anabolic process. At any given time you are in one or the other.
So while you can preserve muscle while losing fat, or minimize fat gain while losing muscle you will not directly replace fat with muscle.0 -
touche.Because as previously stated, gaining muscle on a cut is not feasible.
Oh and...
Fat does not "convert to muscle".why not use the mass you already have and just convert it to muscle...?
no obviously it doesn't actually convert, it's just a turn of phrase.
but if your body has other fuel sources to burn besides your muscle tissue, it will burn them, thus shedding fat at the same time as your lifting heavy builds muscle size and strength
Your body doesn't work like that. Burning fat is a catabolic process, gaining muscle is an anabolic process. At any given time you are in one or the other.
So while you can preserve muscle while losing fat, or minimize fat gain while losing muscle you will not directly replace fat with muscle.0 -
Kristian, do please tell us what you ate on this so called unhealthy diet where weight loss didn't occur or was slow?? I know lots of us would love to know. Thanks.0
-
I did some interesting reading, about doing HIIT (High Intensity Interval Training) while in ketosis. Saying that it could, cause your body could to be catabolic. I was wondering if anyone could shed some more light on this. Try and keep this civil, thank you.0
-
A typical high-fat/low-carb/moderate-protein is no worse or better at preserving lean mass. However there is considerable evidence - as Lyle McDonald get's into in both his book "The Ketogenic Diet" and on his website, showing that a higher protein version of the diet is a very appropriate choice for body recomposition.ketogenic diets in general aren't that great for preserving muscle mass.
This is not necessarily true. I always do my HIIT starting about 30-45 minutes after ingestion of my highest-carb meal of the day - typically 15 to 20g of carbohydrate for me. This ensures there is enough circulating glucose in the system to fuel the HIIT.If you do HIIT then more protein will get converted to glucose and used for energy. This will come from muscle protein.
Also of note, although ketogenic dieters have reduced glycogen stores compared to non-keto dieters, they still have enough to fuel HIIT exercise at reasonable levels; even moreso for those that choose to do a CKD (cyclic ketogenic diet) which is excellent for fat-loss with retention of lean muscle-mass, as all research indicates.
Anaerobic exercise can ONLY use glucose for it's metabolism, so yes it DOES burn carbs/glycogen - which is the opposite of what you state above.It's a bit more cmoplex than this, because HIIT is anaerobic doesn't burn carbs(glycogen) so much... but hopefully you get the **** of it.
Also, it would only be in extreme circumstances an individual catabolizes lean tissue to support this. Most dieters on MFP are not capable of the effort required to actually get into a zero-glycogen state, let-alone continue to exercise after-such to start catabolizing lean tissue.0 -
How do you figure that?Through out your post it seems like you're talking about a non ketogenic diet.
There's extremely limited creatine phosphate in muscles for any anaerobic exercise, certainly not enough for HIIT. Creatine phosphate is completely metabolized in between 2 and 5 seconds... Not enough to sustain the 20+ seconds required in each proper HIIT protocol interval. Glucose is the primary fuel in anaerobic metabolism, and always will be.About the anerobic pathway, I am thinking along the lines of the creatine phosphate system. Glucose is involved but not directly.
The body typically relies on glycolysis for anaerobic respiration once creatine phosphate is used-up (which as I said, happens very quickly). Glycolysis uses glucose directly, and we can't maintain long term due anaerobic activity due to our lactate threshold, NOT because the process doesn't use glucose, because it does.As you know if glucose was involved directly we would be able to sprint at our max for a good amount of time 10-20mins, it's just not reality.0 -
HIIT is a full gallop and 3 sessions of 30 seconds each would have you wasted for hours after. Take a look at 100 meter sprinters, they could never sustain that pace for much more than 10 seconds, that's HIIT. Even 30 seconds is a stretch of the definition.
How do you figure that?Through out your post it seems like you're talking about a non ketogenic diet.
There's extremely limited creatine phosphate in muscles for any anaerobic exercise, certainly not enough for HIIT. Creatine phosphate is completely metabolized in between 2 and 5 seconds... Not enough to sustain the 20+ seconds required in each proper HIIT protocol interval. Glucose is the primary fuel in anaerobic metabolism, and always will be.About the anerobic pathway, I am thinking along the lines of the creatine phosphate system. Glucose is involved but not directly.
The body typically relies on glycolysis for anaerobic respiration once creatine phosphate is used-up (which as I said, happens very quickly). Glycolysis uses glucose directly, and we can't maintain long term due anaerobic activity due to our lactate threshold, NOT because the process doesn't use glucose, because it does.As you know if glucose was involved directly we would be able to sprint at our max for a good amount of time 10-20mins, it's just not reality.
I see big problem in our little discussion. 1 "what type of HIIT are we talking about?" Some intervals are short, some our long. Depends which ones you do will determine the pathway of course.
Yes i know the CP system runs out really quickly. I know what you're saying but when lactic acid is involved that's when the lactic acid system kicks in and buffering of lactic acid happens.
My example was a person sprinting. I said, "As you know if glucose was involved directly we would be able to sprint at our max for a good amount of time 10-20mins, it's just not reality." We can sprint for a short period of time, befure the quicker energy systems crash, then the glycogen system kicks in. Now you will be using the lactate acid system which can carry you for a little while before you have to slow down. I am just trying to say that youc an't run at a ATP, CP, speed for the distance of a the lactate buffering system. That initially in these quick systems glycogen won't be used until the ATP and CP system crash, then glycogen will be used.0 -
bump. must read entire thread!0
-
A typical high-fat/low-carb/moderate-protein is no worse or better at preserving lean mass. However there is considerable evidence - as Lyle McDonald get's into in both his book "The Ketogenic Diet" and on his website, showing that a higher protein version of the diet is a very appropriate choice for body recomposition.ketogenic diets in general aren't that great for preserving muscle mass.
This is not necessarily true. I always do my HIIT starting about 30-45 minutes after ingestion of my highest-carb meal of the day - typically 15 to 20g of carbohydrate for me. This ensures there is enough circulating glucose in the system to fuel the HIIT.If you do HIIT then more protein will get converted to glucose and used for energy. This will come from muscle protein.
Also of note, although ketogenic dieters have reduced glycogen stores compared to non-keto dieters, they still have enough to fuel HIIT exercise at reasonable levels; even moreso for those that choose to do a CKD (cyclic ketogenic diet) which is excellent for fat-loss with retention of lean muscle-mass, as all research indicates.
Anaerobic exercise can ONLY use glucose for it's metabolism, so yes it DOES burn carbs/glycogen - which is the opposite of what you state above.It's a bit more cmoplex than this, because HIIT is anaerobic doesn't burn carbs(glycogen) so much... but hopefully you get the **** of it.
Also, it would only be in extreme circumstances an individual catabolizes lean tissue to support this. Most dieters on MFP are not capable of the effort required to actually get into a zero-glycogen state, let-alone continue to exercise after-such to start catabolizing lean tissue.
I do agree the higher the protein the better it will be at preserving muscle mass. But we're looking at a ketogenic diet, not a low carb diet.
Through out your post it seems like you're talking about a non ketogenic diet. About the anerobic pathway, I am thinking along the lines of the creatine phosphate system. Glucose is involved but not directly. As you know if glucose was involved directly we would be able to sprint at our max for a good amount of time 10-20mins, it's just not reality. I was tired, and i don't ike getting to much in to details with people on mfp who posts. I just try to keep it simple. As you know sometimes simplicity leaves things out.
Pu, keto and low carb are essentially the same. When I reference my forms of dieting I'm going almost exclusively from Lyle McDonald's work, but Atkins does put someone in ketosis. Where Atkins (and plenty of other low carb diets) go very wrong, is that many aren't very technical. Many of them don't explain the first "big drop" is a glycogen related fluid shift, and simply go by "eat when you're hungry". Which is partly why some people in general think keto is the "all you can eat bacon diet".
Now with the glygocen storage thing:
Even someone doing a SKD (with no carb ups) is still going to have SOME muscle glycogen, although it's typically lower than the other forms. Whereas a CKD (with carb ups) takes advantage of glycogen supercompensation. Hormonal issues aside, the primary reason for carbups is energy.
It then become something of a catch 22 scenario (regarding keto). If someone is actually cognizant of glycogen and performance, they're also likely to be on a CKD for the same reason. What a person is actually doing is going to dictate what they should be doing diet wise.0 -
Haven't heard carb up and supercompensation mentioned for a while. 10 points.
A typical high-fat/low-carb/moderate-protein is no worse or better at preserving lean mass. However there is considerable evidence - as Lyle McDonald get's into in both his book "The Ketogenic Diet" and on his website, showing that a higher protein version of the diet is a very appropriate choice for body recomposition.ketogenic diets in general aren't that great for preserving muscle mass.
This is not necessarily true. I always do my HIIT starting about 30-45 minutes after ingestion of my highest-carb meal of the day - typically 15 to 20g of carbohydrate for me. This ensures there is enough circulating glucose in the system to fuel the HIIT.If you do HIIT then more protein will get converted to glucose and used for energy. This will come from muscle protein.
Also of note, although ketogenic dieters have reduced glycogen stores compared to non-keto dieters, they still have enough to fuel HIIT exercise at reasonable levels; even moreso for those that choose to do a CKD (cyclic ketogenic diet) which is excellent for fat-loss with retention of lean muscle-mass, as all research indicates.
Anaerobic exercise can ONLY use glucose for it's metabolism, so yes it DOES burn carbs/glycogen - which is the opposite of what you state above.It's a bit more cmoplex than this, because HIIT is anaerobic doesn't burn carbs(glycogen) so much... but hopefully you get the **** of it.
Also, it would only be in extreme circumstances an individual catabolizes lean tissue to support this. Most dieters on MFP are not capable of the effort required to actually get into a zero-glycogen state, let-alone continue to exercise after-such to start catabolizing lean tissue.
I do agree the higher the protein the better it will be at preserving muscle mass. But we're looking at a ketogenic diet, not a low carb diet.
Through out your post it seems like you're talking about a non ketogenic diet. About the anerobic pathway, I am thinking along the lines of the creatine phosphate system. Glucose is involved but not directly. As you know if glucose was involved directly we would be able to sprint at our max for a good amount of time 10-20mins, it's just not reality. I was tired, and i don't ike getting to much in to details with people on mfp who posts. I just try to keep it simple. As you know sometimes simplicity leaves things out.
Pu, keto and low carb are essentially the same. When I reference my forms of dieting I'm going almost exclusively from Lyle McDonald's work, but Atkins does put someone in ketosis. Where Atkins (and plenty of other low carb diets) go very wrong, is that many aren't very technical. Many of them don't explain the first "big drop" is a glycogen related fluid shift, and simply go by "eat when you're hungry". Which is partly why some people in general think keto is the "all you can eat bacon diet".
Now with the glygocen storage thing:
Even someone doing a SKD (with no carb ups) is still going to have SOME muscle glycogen, although it's typically lower than the other forms. Whereas a CKD (with carb ups) takes advantage of glycogen supercompensation. Hormonal issues aside, the primary reason for carbups is energy.
It then become something of a catch 22 scenario (regarding keto). If someone is actually cognizant of glycogen and performance, they're also likely to be on a CKD for the same reason. What a person is actually doing is going to dictate what they should be doing diet wise. 0
0 -
A typical high-fat/low-carb/moderate-protein is no worse or better at preserving lean mass. However there is considerable evidence - as Lyle McDonald get's into in both his book "The Ketogenic Diet" and on his website, showing that a higher protein version of the diet is a very appropriate choice for body recomposition.ketogenic diets in general aren't that great for preserving muscle mass.
This is not necessarily true. I always do my HIIT starting about 30-45 minutes after ingestion of my highest-carb meal of the day - typically 15 to 20g of carbohydrate for me. This ensures there is enough circulating glucose in the system to fuel the HIIT.If you do HIIT then more protein will get converted to glucose and used for energy. This will come from muscle protein.
Also of note, although ketogenic dieters have reduced glycogen stores compared to non-keto dieters, they still have enough to fuel HIIT exercise at reasonable levels; even moreso for those that choose to do a CKD (cyclic ketogenic diet) which is excellent for fat-loss with retention of lean muscle-mass, as all research indicates.
Anaerobic exercise can ONLY use glucose for it's metabolism, so yes it DOES burn carbs/glycogen - which is the opposite of what you state above.It's a bit more cmoplex than this, because HIIT is anaerobic doesn't burn carbs(glycogen) so much... but hopefully you get the **** of it.
Also, it would only be in extreme circumstances an individual catabolizes lean tissue to support this. Most dieters on MFP are not capable of the effort required to actually get into a zero-glycogen state, let-alone continue to exercise after-such to start catabolizing lean tissue.
I do agree the higher the protein the better it will be at preserving muscle mass. But we're looking at a ketogenic diet, not a low carb diet.
Through out your post it seems like you're talking about a non ketogenic diet. About the anerobic pathway, I am thinking along the lines of the creatine phosphate system. Glucose is involved but not directly. As you know if glucose was involved directly we would be able to sprint at our max for a good amount of time 10-20mins, it's just not reality. I was tired, and i don't ike getting to much in to details with people on mfp who posts. I just try to keep it simple. As you know sometimes simplicity leaves things out.
Pu, keto and low carb are essentially the same. When I reference my forms of dieting I'm going almost exclusively from Lyle McDonald's work, but Atkins does put someone in ketosis. Where Atkins (and plenty of other low carb diets) go very wrong, is that many aren't very technical. Many of them don't explain the first "big drop" is a glycogen related fluid shift, and simply go by "eat when you're hungry". Which is partly why some people in general think keto is the "all you can eat bacon diet".
Now with the glygocen storage thing:
Even someone doing a SKD (with no carb ups) is still going to have SOME muscle glycogen, although it's typically lower than the other forms. Whereas a CKD (with carb ups) takes advantage of glycogen supercompensation. Hormonal issues aside, the primary reason for carbups is energy.
It then become something of a catch 22 scenario (regarding keto). If someone is actually cognizant of glycogen and performance, they're also likely to be on a CKD for the same reason. What a person is actually doing is going to dictate what they should be doing diet wise.
While I'm not on Atkins, I have read the book cover to cover several times. He mentions the fluid shift on multiple occasions.0 -
Technically, any protocol longer than 30 seconds is not (in my opinion) true HIIT.I see big problem in our little discussion. 1 "what type of HIIT are we talking about?" Some intervals are short, some our long. Depends which ones you do will determine the pathway of course.
HIIT is all-out, maximum-intensity effort for 20-30 seconds. If you can sustain the effort more than 20-30 seconds, it's technically not HIIT, it's just interval training - in my opinion. (There is currently no "standard" to define HIIT)
Longer than 30 seconds is generally well-under 100% VO2 max. Some 60 second protocols are designed for 90-95% VO2 max (even less for those who are sedentary/obese), and based on what I've seen this can actually be very beneficial for improvements in insulin-sensitivity, but perhaps not as good for body-composition/fat-loss as higher-intensity interval training.
One reason so many that are choosing a low-carb/ketogenic diet augmented with HIIT is because they are insulin-resistant, and this particular combination of diet and exercise regime is - simply put - vastly superior to any others in improving this metabolic condition.0 -
Yes, glycolysis is happening almost immediately. Seriously, most of us have a maximum of a few (2-5) seconds worth of creatine phosphate. So for a 20-30 second sprint, between 70 and 90% of it is utilizing glucose for ATP production, not creatine phosphate. After the first sprint it's basically all glucose, which comes from glycolysis.Okay following that definition, you're still saying the lactic acid system kicks in initially? The lactic acid system kicks in once the quicker systems are depleted.
Though we CAN generate glucose via gluconeogenesis which could catabolize lean tissue, this just doesn't happen in the case of HIIT. Gluconeogenesis isn't efficient enough to quickly provide the necessary glucose for cellular respiration in anaerobic metabolism. Glycolysis is.
Big differences: Essentially all of the body's cells are able to perform glycolysis (which is the first step in metabolism of glucose taken up via transporters in the cell membrane), whereas gluconeogenesis takes place primarily in liver cells. Glycolysis starts with glucose and ends with pyruvate AND generates ATP whereas gluconeogenesis has cells consume ATP to regenerate glucose from pyruvate, so there's actually a net-loss of energy with gluconeogenesis and a net-gain with glycolysis.
Because it results in increased energy availability for the cell, glycolysis increases when the cell is in need of energy.
If someone suggested to you that gluconeogenesis supports any anaerobic activity instantaneously, they're simply incorrect.0 -
A typical high-fat/low-carb/moderate-protein is no worse or better at preserving lean mass. However there is considerable evidence - as Lyle McDonald get's into in both his book "The Ketogenic Diet" and on his website, showing that a higher protein version of the diet is a very appropriate choice for body recomposition.ketogenic diets in general aren't that great for preserving muscle mass.
This is not necessarily true. I always do my HIIT starting about 30-45 minutes after ingestion of my highest-carb meal of the day - typically 15 to 20g of carbohydrate for me. This ensures there is enough circulating glucose in the system to fuel the HIIT.If you do HIIT then more protein will get converted to glucose and used for energy. This will come from muscle protein.
Also of note, although ketogenic dieters have reduced glycogen stores compared to non-keto dieters, they still have enough to fuel HIIT exercise at reasonable levels; even moreso for those that choose to do a CKD (cyclic ketogenic diet) which is excellent for fat-loss with retention of lean muscle-mass, as all research indicates.
Anaerobic exercise can ONLY use glucose for it's metabolism, so yes it DOES burn carbs/glycogen - which is the opposite of what you state above.It's a bit more cmoplex than this, because HIIT is anaerobic doesn't burn carbs(glycogen) so much... but hopefully you get the **** of it.
Also, it would only be in extreme circumstances an individual catabolizes lean tissue to support this. Most dieters on MFP are not capable of the effort required to actually get into a zero-glycogen state, let-alone continue to exercise after-such to start catabolizing lean tissue.
I do agree the higher the protein the better it will be at preserving muscle mass. But we're looking at a ketogenic diet, not a low carb diet.
Through out your post it seems like you're talking about a non ketogenic diet. About the anerobic pathway, I am thinking along the lines of the creatine phosphate system. Glucose is involved but not directly. As you know if glucose was involved directly we would be able to sprint at our max for a good amount of time 10-20mins, it's just not reality. I was tired, and i don't ike getting to much in to details with people on mfp who posts. I just try to keep it simple. As you know sometimes simplicity leaves things out.
Pu, keto and low carb are essentially the same. When I reference my forms of dieting I'm going almost exclusively from Lyle McDonald's work, but Atkins does put someone in ketosis. Where Atkins (and plenty of other low carb diets) go very wrong, is that many aren't very technical. Many of them don't explain the first "big drop" is a glycogen related fluid shift, and simply go by "eat when you're hungry". Which is partly why some people in general think keto is the "all you can eat bacon diet".
Now with the glygocen storage thing:
Even someone doing a SKD (with no carb ups) is still going to have SOME muscle glycogen, although it's typically lower than the other forms. Whereas a CKD (with carb ups) takes advantage of glycogen supercompensation. Hormonal issues aside, the primary reason for carbups is energy.
It then become something of a catch 22 scenario (regarding keto). If someone is actually cognizant of glycogen and performance, they're also likely to be on a CKD for the same reason. What a person is actually doing is going to dictate what they should be doing diet wise.
Ketogenic diet is determined by the ketone concentration in the blood. Doing a low carb doesn't necessarily mean you will be in ketosis. If you do low carb you can eat a ton of protein which can throw you out of ketosis.
You're right, but the actual amount of protein most people have to eat for that is pretty high. There's people out there that DO bulk on keto with a protein intake of around 2g/lbm.
You said it yourself, someone needs to eat a ton of protein for gluconeogenis to the be primary energy source (and of course both carbs and fats would likely have to be absent as well).
You can be as nit picky as you want with it, but essentially anyone eating low carb is also going to be in ketosis.0 -
That's awesome!
I'm sleeping all night, not only am I sleeping all night but I'm sleeping HARD! I love it!
This is the best part of keto for me. I sleep the whole night. I don't wake up AT ALL. Doesn't mater what time I go to bed, I always wake up at 5:30 am and I feel rested. That never happened before keto. I have done two Carb Feed days in 4 months and I gotta tell you that I felt like **** and slept like **** afterwards. I was trying out the CKD version of the ketogenic diet and as great as I felt during my workout, being able to lift and go for an hour with no problem, the side effects were not worth it (not sleeping well, waking up the next day with a migraine, thirst like nobodies business and stomach issues)0 -
Keto is garbage. It tricks people into thinking they doing some crazy thing with their body but in reality all Keto is is a calorie restriction in disguise. Low carb does help to lose water weight and glycogen which can be good to lose some quick pounds.0
-
all Keto is is a calorie restriction in disguise.
Oh really? Is that all it is? Please sir, tell us more!0 -
Let me see. almost half of all protein gets converted to glucose. For every gram of protein consume 48% of it gets converted to glucose. The brain uses about 100g, so you need more than 100g to not be in ketosis. To consume 102g of glucose assuming you're eating 30g of carbs a day. You need to eat 150g of protein. That's enough to throw you out of ketosis consuming 30g of net carbs.
I would love to see where you're getting your numbers, because your're simply wrong. Gluconogenesis has been repeatedly been shown to be stable under varying levels of intake.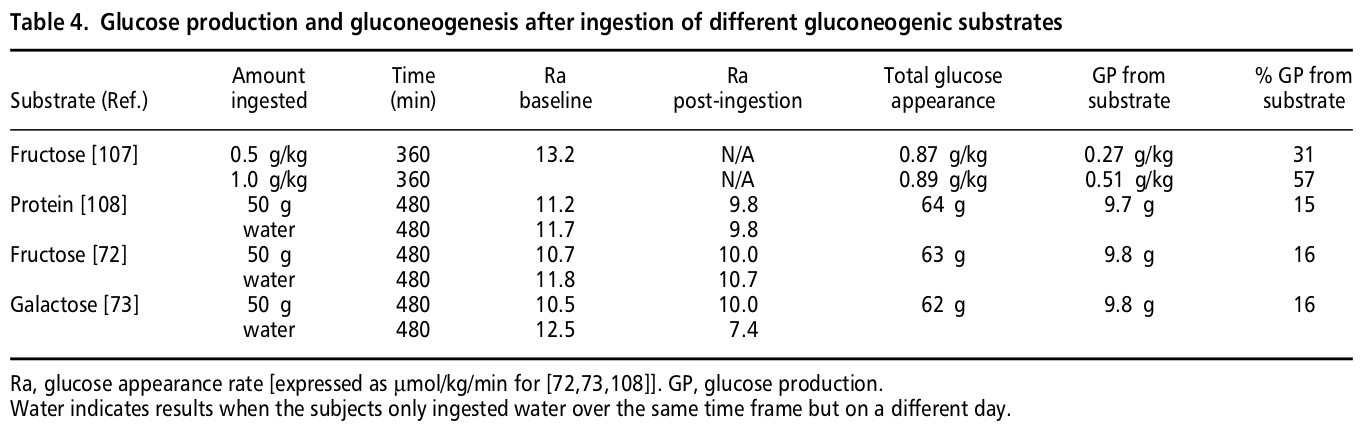
The fate of amino acids deaminated following protein ingestion is uncertain. Presumably, the majority of the carbon skeletons of the amino acids are converted into glucose in the liver. In the present study, tritiated glucose dilution tracer studies have been used to determine the effect of a protein meal on the glucose appearance rate in plasma. Five normal male subjects ingested 50 g of protein in the form of cottage cheese. The glucose appearance rate was determined using a constant infusion of 3H-glucose, and compared to the glucose appearance rate following the ingestion of just water in the same subjects over an 8-hour period. The total amount of protein deaminated and converted to urea also was quantitated. Urea production could account for the metabolism of 29.3 g of protein ingested, or 58.5%. Glucose appearing in the circulation as a result of amino acid metabolism determined by tracer methodology was 9.68 +/- 5.7 g. Based on the gluconeogenic potential of cottage cheese (42.3 g of glucose from 50 g of cottage cheese protein), this could only account for at most 43% of protein metabolized, or 23% of the total amount of protein ingested. The fate of the remaining amino acids metabolized remains to be determined.
http://www.jacn.org/content/11/6/701.abstract0 -
all Keto is is a calorie restriction in disguise.
Oh really? Is that all it is? Please sir, tell us more!
bro stop while you're way behind. it's a good way for you to lose all your muscle mass.0 -
all Keto is is a calorie restriction in disguise.
Oh really? Is that all it is? Please sir, tell us more!
Im not going to go into the details of ketosis or how using ketones for energy ect ect. Because I believe it is an unhealthy and stressful way to lose weight. I should have been less blunt and gave a better option but Im tired of hearing about Keto. Altho if youd like to "educate" me with your knowledge and out of this world physique please do so.0 -
A typical high-fat/low-carb/moderate-protein is no worse or better at preserving lean mass. However there is considerable evidence - as Lyle McDonald get's into in both his book "The Ketogenic Diet" and on his website, showing that a higher protein version of the diet is a very appropriate choice for body recomposition.ketogenic diets in general aren't that great for preserving muscle mass.
This is not necessarily true. I always do my HIIT starting about 30-45 minutes after ingestion of my highest-carb meal of the day - typically 15 to 20g of carbohydrate for me. This ensures there is enough circulating glucose in the system to fuel the HIIT.If you do HIIT then more protein will get converted to glucose and used for energy. This will come from muscle protein.
Also of note, although ketogenic dieters have reduced glycogen stores compared to non-keto dieters, they still have enough to fuel HIIT exercise at reasonable levels; even moreso for those that choose to do a CKD (cyclic ketogenic diet) which is excellent for fat-loss with retention of lean muscle-mass, as all research indicates.
Anaerobic exercise can ONLY use glucose for it's metabolism, so yes it DOES burn carbs/glycogen - which is the opposite of what you state above.It's a bit more cmoplex than this, because HIIT is anaerobic doesn't burn carbs(glycogen) so much... but hopefully you get the **** of it.
Also, it would only be in extreme circumstances an individual catabolizes lean tissue to support this. Most dieters on MFP are not capable of the effort required to actually get into a zero-glycogen state, let-alone continue to exercise after-such to start catabolizing lean tissue.
I do agree the higher the protein the better it will be at preserving muscle mass. But we're looking at a ketogenic diet, not a low carb diet.
Through out your post it seems like you're talking about a non ketogenic diet. About the anerobic pathway, I am thinking along the lines of the creatine phosphate system. Glucose is involved but not directly. As you know if glucose was involved directly we would be able to sprint at our max for a good amount of time 10-20mins, it's just not reality. I was tired, and i don't ike getting to much in to details with people on mfp who posts. I just try to keep it simple. As you know sometimes simplicity leaves things out.
Pu, keto and low carb are essentially the same. When I reference my forms of dieting I'm going almost exclusively from Lyle McDonald's work, but Atkins does put someone in ketosis. Where Atkins (and plenty of other low carb diets) go very wrong, is that many aren't very technical. Many of them don't explain the first "big drop" is a glycogen related fluid shift, and simply go by "eat when you're hungry". Which is partly why some people in general think keto is the "all you can eat bacon diet".
Now with the glygocen storage thing:
Even someone doing a SKD (with no carb ups) is still going to have SOME muscle glycogen, although it's typically lower than the other forms. Whereas a CKD (with carb ups) takes advantage of glycogen supercompensation. Hormonal issues aside, the primary reason for carbups is energy.
It then become something of a catch 22 scenario (regarding keto). If someone is actually cognizant of glycogen and performance, they're also likely to be on a CKD for the same reason. What a person is actually doing is going to dictate what they should be doing diet wise.
Ketogenic diet is determined by the ketone concentration in the blood. Doing a low carb doesn't necessarily mean you will be in ketosis. If you do low carb you can eat a ton of protein which can throw you out of ketosis.
You're right, but the actual amount of protein most people have to eat for that is pretty high. There's people out there that DO bulk on keto with a protein intake of around 2g/lbm.
You said it yourself, someone needs to eat a ton of protein for gluconeogenis to the be primary energy source (and of course both carbs and fats would likely have to be absent as well).
You can be as nit picky as you want with it, but essentially anyone eating low carb is also going to be in ketosis.
Let me see. almost half of all protein gets converted to glucose. For every gram of protein consume 48% of it gets converted to glucose. The brain uses about 100g, so you need more than 100g to not be in ketosis. To consume 102g of glucose assuming you're eating 30g of carbs a day. You need to eat 150g of protein. That's enough to throw you out of ketosis consuming 30g of net carbs.
Your glucose conversion rate is the MAXIMUM, not the norm.
Once someone is keto-adapted the brain's reliance on glucose drops to approximately 25%. Those macros you listed are almost identical to what my daily intake was when I was doing an SKD (150g protein, 30g net carbs) and I had no trouble maintaining ketosis for months at a time.
GNG is a highly inefficient process, and really only utilized in some extreme cases.
here's lyle's own word though:
As long term adaptation to ketosis continues, there are a number of adaptations which
occur to further spare glucose. From the third day of ketosis to three weeks of fasting, the brain
gradually increases its use of ketones for fuel, ultimately deriving up to 75% of its total energy
from ketones (6,26). This shift to using ketones by the brain means that only 40 grams of
glucose per day is required, the remaining 60-75 grams of energy being provided by ketones (26).
This means that less protein must be broken down to produce glucose. Since TG breakdown will
still provide 18 grams of glucose per day, protein breakdown will only be 20 grams per day (see
table 2 on the next page) (6). As stated previously, is appears the primary purpose of ketones in
humans is to provide the brain with a non-glucose, fat-derived fuel for the brain (27,30).0 -
all Keto is is a calorie restriction in disguise.
Oh really? Is that all it is? Please sir, tell us more!
bro stop while you're way behind. it's a good way for you to lose all your muscle mass.
Let him be. Im usually all for helping someone out but its obvious he has it all figured out and wants to attempt to flame someone who knows 10x the amount he does and actually can back up his knowledge with results.0 -
Lyle has A LOT OF useful information! Altho EVERYONE seems to only want to read the Ketogenic diet or the rapid fat loss handbook. Nobody wants to read the guide to flexible dieting because EVERYONE wants a quick fix without hard work. Keto works. Its proven. Is it sustainable if you can manage to not go carb crazy before u even reach Ketosis assuming u even get their in the first place? Not for most.0













This discussion has been closed.
Categories
- All Categories
- 1.4M Health, Wellness and Goals
- 398.2K Introduce Yourself
- 44.7K Getting Started
- 261K Health and Weight Loss
- 176.4K Food and Nutrition
- 47.7K Recipes
- 233K Fitness and Exercise
- 462 Sleep, Mindfulness and Overall Wellness
- 6.5K Goal: Maintaining Weight
- 8.7K Goal: Gaining Weight and Body Building
- 153.5K Motivation and Support
- 8.4K Challenges
- 1.4K Debate Club
- 96.5K Chit-Chat
- 2.6K Fun and Games
- 4.8K MyFitnessPal Information
- 12 News and Announcements
- 21 MyFitnessPal Academy
- 1.5K Feature Suggestions and Ideas
- 3.2K MyFitnessPal Tech Support Questions