Coronavirus prep
Replies
-
lynn_glenmont wrote: »GaleHawkins wrote: »T1DCarnivoreRunner wrote: »baconslave wrote: »MikePfirrman wrote: »The Tuscaloosa Alabama story -- students having Covid-19 parties, with a known infected person, putting money into a pot and the first one to officially "get it" gets the money -- makes me believe that we are the dumbest country in history. Sorry, there's no other way to look at it.
Went out to another outdoor concert last night, much better band this time. AZ rates are soaring. Only states worse are TX and CA, where my kids live! We went out again last night to eat and ate on a patio again.
I've resigned myself that there is no "back to normal" unless they find a vaccine for this. Or it could mutate so much that it won't be nearly as deadly. But once school is back in session, in the Fall, which I think is a terrible idea BTW, 1.5M dead doesn't seem too outrageous now. Perhaps 2M. The numbers don't lie. 5% have been infected and 130K dead. Multiply X 13. That's the point at which they say we will have herd immunity.
Our response as a country has been a pathetic combination of finger pointing, selfishness and incompetence.
Yep.
My sister lives in Houston, and I'm here in northeast TN, which is itchin' to catch up to TX. We have in this country a large population of entitled, uncaring, thoughtless, brats of widely varying ages. I have friends (30s & 40s), inlaws (60s), a 19-year-old sister-in-law, aunts and uncles (50s-70s) who are being so belligerent, selfish and ignorant. They are proof that unfortunately we can't just blame the lack of leadership of our government. Though they have certainly contributed greatly.
Totally agree. We need a national mask law with steep penalties. And strict enforcement.
With no or reduced funding for enforcement in the USA who's going to be the enforcement ?
Enforcement doesn't have to take the form of immediate physical restraint , tasering, and/or arrest. It can be in the form of consequences, such as "no-shop" lists like the "no-fly" lists airlines are saying they'll use for customers who won't wear masks. "No shirt, no shoes, no mask, no service."
Exactly!! That's how it is where I live. It is impossible to enter any retail store without a mask. You simply won't be allowed inside. This along with the temperature check and hand sanitizer stations at the door.
Here too where they have the resources for that (large chain stores, my local grocery and 7-11 (where cops hang out, I think it's one of the bathrooms they use), and of course buildings downtown). I think local stores have problems enforcing, since they don't have enough employees to dedicate to monitoring that or security. I haven't seen problems inside stores here, but have seen videos from all over the US showing non compliant morons. We also generally have hand sanitizers at the door and are wiping off carts and baskets.
The temperature check thing we are doing at my office and I think it's kind of stupid. First of all, I don't think the forehead thermometers are actually accurate, and second, many are contagious without temperatures and if you have a temperature you likely have symptoms.4 -
baconslave wrote: »MikePfirrman wrote: »The Tuscaloosa Alabama story -- students having Covid-19 parties, with a known infected person, putting money into a pot and the first one to officially "get it" gets the money -- makes me believe that we are the dumbest country in history. Sorry, there's no other way to look at it.
Went out to another outdoor concert last night, much better band this time. AZ rates are soaring. Only states worse are TX and CA, where my kids live! We went out again last night to eat and ate on a patio again.
I've resigned myself that there is no "back to normal" unless they find a vaccine for this. Or it could mutate so much that it won't be nearly as deadly. But once school is back in session, in the Fall, which I think is a terrible idea BTW, 1.5M dead doesn't seem too outrageous now. Perhaps 2M. The numbers don't lie. 5% have been infected and 130K dead. Multiply X 13. That's the point at which they say we will have herd immunity.
Our response as a country has been a pathetic combination of finger pointing, selfishness and incompetence.
Yep.
My sister lives in Houston, and I'm here in northeast TN, which is itchin' to catch up to TX. We have in this country a large population of entitled, uncaring, thoughtless, brats of widely varying ages. I have friends (30s & 40s), inlaws (60s), a 19-year-old sister-in-law, aunts and uncles (50s-70s) who are being so belligerent, selfish and ignorant. They are proof that unfortunately we can't just blame the lack of leadership of our government. Though they have certainly contributed greatly.
I'm so sorry. I'd pick you up and bring you here. No cases for now till the tourists show up I'm guessing. Everyone wants to come to Queensland worst luck. Hoping we keep boarders closed. Doubt it'll happen. Yeah.. come up and give us Covid.
You can open the borders but put restrictions in place. We expect tourists from next week, but they MUST have a test before traveling, and bring a COVID-free certificate to show at Immigration and Customs.
I take it by the reference to Immigration and Customs that you are talking about international tourists.
Australia, where mockchoc and I live, is a long way from accepting international tourists.
I think mockchoc was talking more state borders , especially since she said ' come up and give us Covid ' ie come up from southern states NSW and Victoria where Covid is still very active.
safe states here have closed their borders to other states - we may start opening to other safe states at some point.
I would like to go on holiday to Whitsunday islands ( northern Queensland) - may be possible in a few months from South Australia, also safe state.
3 -
This outrageous!!!
Woman spits on 7-Eleven counter after being asked to wear a mask
https://www.usatoday.com/story/money/2020/07/02/7-eleven-mask-incident-viral-video-spits-counter/5368869002/
https://freekeene.com/2020/06/29/porcfest-2020-is-over-is-today-the-eighth-or-first-day-of-forkfest-2020-you-decide/
Yessiree, people like her and the ones who openly attend events as posted in this newspaper......they certainly can be trusted to do what's right.
When I first heard about the Porcfest Freedom Festival, I was wondering what kind of people attended and what their objectives were. After reading the comments, I got a good impression.
I'm expecting our current rates to start jumping all over the effin place. NH and VT are scenic, quiet, serene places to live and watching tourism boom right now, with people fleeing the cities and chaos of life for here.....makes me extremely nervous. Covid-19 is NOT going to sneak away or die down(despite what some leaders say!!) without people's adhering to some common sense. And obviously, some people have zero.
NH and VT are scenic, quiet, serene places to live and watching tourism boom right now, with people fleeing the cities and chaos of life for here.....makes me extremely nervous. Covid-19 is NOT going to sneak away or die down(despite what some leaders say!!) without people's adhering to some common sense. And obviously, some people have zero.
PLEASE don't be so selfish through all of this to only think of yourselves. You are living in a world with other humans. That entitlement of some that we always hear about? Going to be the death of us. 7 -
ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.1 -
Didn't you post that yesterday?
I think we've already acknowledged that the non-pharmaceutical methods (and not just face masks) are not 100% effective. Even if they're only 5% effective, that's 5% more people NOT getting sick.
It's not a perfect solution.
There is no perfect solution.
We're just trying to space out the infection rate so everything doesn't go to Hell in a handbasket at once.
16 -
Those studies all acknowledge the imperfect data collection, too.
Virtually the ONLY non-pharm intervention that IS possible to mandate is mask wearing. So at least it would keep people thinking about this if they're seeing masks everywhere.
It's not going to be forever. What's the big deal about wearing a mask in a store??10 -
(snip)
But more importantly, the bean situation in my area has been terrible since this started. I saw an interesting Patriot Act episode on our supply chain being too efficient which makes it unable to handle these types of shocks.
Just my opinion, but: I think it may be more productive to think of those supply chains as "insufficiently resilient", which - when evaluating their effectiveness over a span of time, especially - is an example of not being efficient enough under real-world conditions.
If we learn from all this, we have an opportunity to improve, building in resilience while maintaining at least some of the reduced inventory and other features of the system that's proven flawed.
IMO, improvement happens in cycles. JIT manufacturing was an improvement. We can improve the improvement; backtracking is not necessarily the only solution. (And I know the PP didn't say or imply that it was - I'm just riffing off the post, not completely disagreeing with it.)2 -
ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
Without disputing the conclusion at all**, I'd observe that the research is influenza research. Is Covid transmitted identically (same droplet size needed in exhalates for transmission, and that sort of thing), same volume of virus bits needed to infect, same effect of environmentals (heat, light, airflow) on life of virus or other aspects that make it more/less contagious via exhalation, etc.?
I have no idea. Could be identical. Could be not identical. Just because it's a symptomatically similar disease, doesn't make the different virus have the same transmission characteristics, AFAIK.
It does seem to me that some of what had the experts confused and sending mixed messages, certainly at first but to some extent even now, was that research on factors like those I mentioned were just beginning to be to be published for this specific virus.
I'd also observe that there's some sign that countries with high mask adherence had better virus control, generally (possibly not absolutely). That's a correlational thing, so weak evidence . . . but wearing a mask is pretty easy & cheap, so seems worth doing even if there's some mere correlational findings as the justification. (I understand that some people with health issues can have problems wearing masks. I'm talking in general terms about the population.)
From my amateur history of closely reading other health research (breast cancer), it seems to me that preventatives/treatments with generally no negative side-effects will be accepted as part of standard practice/recommendations based on moderately weak evidence; and things that are more likely to cause harm are subjected to higher standards for proof of effectiveness before becoming standard practice. Outside of the health-related minority end-cases, mask wearing is pretty harmless.
** Not because I think it's indisputable, but because I'm not an expert, and I don't feel like researching/disputing today. 9
9 -
ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
I'm not sure it's the same as influenza. We know Coronavirus is spread by droplets leaving our mouth and nose, so it is logical that a mask that limits droplets will work. Is it 100%? Nope. Nobody ever said it is... but any effectiveness is worthwhile.
In fact, unless if a mask was proven to be 0% effective (not against influenza), they should be required. Even a 1% decrease in spread means more than a thousand lives saved here in the U.S. alone... so far. If you believe your personal convenience is more important than more than 1,000 lives; then just stay home.13 -
T1DCarnivoreRunner wrote: »ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
I'm not sure it's the same as influenza. We know Coronavirus is spread by droplets leaving our mouth and nose, so it is logical that a mask that limits droplets will work. Is it 100%? Nope. Nobody ever said it is... but any effectiveness is worthwhile.
In fact, unless if a mask was proven to be 0% effective (not against influenza), they should be required. Even a 1% decrease in spread means more than a thousand lives saved here in the U.S. alone... so far. If you believe your personal convenience is more important than more than 1,000 lives; then just stay home.
Can you point me in the direction of the current death rate? Google seems to be failing me. I came up with 0.04%, this is all deaths - not taking into account comorbidities and stuff. I'm sure an expert could get me a better number. I'm not sure a 1% or 5% effectiveness rate would be worth mandates or enforcement. Would you take a vaccine with a 1% effectiveness rate?
People die in car crashes every year, should we make more restrictive mandates (10mph speed limits) and spend money on enforcement? It would save significantly more people from death or injury.
Don't get me wrong, I wear a mask where required. My state hasn't made a mandate and I'm glad they haven't. They've done contact tracing, people aren't picking up COVID from the gym or the restaurants. The new cases haven't gotten them there. They are getting them from their household, or from large gatherings I'm guessing where social distancing isn't enforced - like protests and other large gatherings.3 -
people aren't picking up COVID from the gym or the restaurants.
Maybe because of the masks, social distancing and closures people are not getting the virus in gyms and restaurants.
You just shot down your own argument.8 -
ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
Without disputing the conclusion at all**, I'd observe that the research is influenza research. Is Covid transmitted identically (same droplet size needed in exhalates for transmission, and that sort of thing), same volume of virus bits needed to infect, same effect of environmentals (heat, light, airflow) on life of virus or other aspects that make it more/less contagious via exhalation, etc.?
I have no idea. Could be identical. Could be not identical. Just because it's a symptomatically similar disease, doesn't make the different virus have the same transmission characteristics, AFAIK.
It does seem to me that some of what had the experts confused and sending mixed messages, certainly at first but to some extent even now, was that research on factors like those I mentioned were just beginning to be to be published for this specific virus.
I'd also observe that there's some sign that countries with high mask adherence had better virus control, generally (possibly not absolutely). That's a correlational thing, so weak evidence . . . but wearing a mask is pretty easy & cheap, so seems worth doing even if there's some mere correlational findings as the justification. (I understand that some people with health issues can have problems wearing masks. I'm talking in general terms about the population.)
From my amateur history of closely reading other health research (breast cancer), it seems to me that preventatives/treatments with generally no negative side-effects will be accepted as part of standard practice/recommendations based on moderately weak evidence; and things that are more likely to cause harm are subjected to higher standards for proof of effectiveness before becoming standard practice. Outside of the health-related minority end-cases, mask wearing is pretty harmless.
** Not because I think it's indisputable, but because I'm not an expert, and I don't feel like researching/disputing today.
I made it clear it was influenza research, we don't have 70 years of covid research to look at, now do we?
I'm fine with it being a "standard practice/recommendation" that is not the same as a mandate with enforcement.
Mandates, and all this mask-wearing hype (when the science is iffy, at best), it causes discrimination against those who don't. Prejudice. Sanctimonious behavior. Racial discrimination (yes, it has happened). When everyone is hyping it up like if you don't do it, you are gonna kill your grandma - well the science just isn't there.
I'm tired of seeing leaders standing up saying "WEAR YOUR MASKS" and then when they think the camera cuts off, they take it off - if they don't believe it, why are they preaching it? or reporters on the beach saying "No one is wearing masks! The horror!" and a passerby points out their camera guy isn't wearing a mask. It's just becoming a way to point fingers and shame people.2 -
Without disputing the conclusion at all**, I'd observe that the research is influenza research. Is Covid transmitted identically (same droplet size needed in exhalates for transmission, and that sort of thing), same volume of virus bits needed to infect, same effect of environmentals (heat, light, airflow) on life of virus or other aspects that make it more/less contagious via exhalation, etc.?
I have no idea. Could be identical. Could be not identical. Just because it's a symptomatically similar disease, doesn't make the different virus have the same transmission characteristics, AFAIK.
I didn't link it because it was symptomatically similar, I did because it was a respiratory spread virus - not a bacteria (a previous thing posted was a guy looking at bacteria coming past a mask/not ) - I thought a meta-analysis of influenza spread that was on actual people getting actually ill was far closer to what you'd see with another respiratory virus.
I think masks help some, we've had some people sick, like a hairdresser, who saw customers and didn't spread it to them because they wore masks. That kind of one-on-one close contact? Yeah, I think masks will minimize that. Dentists? Yep.
Me walking down a 10ft wide aisle in a grocery store and passing you for 5 seconds without a mask? Not likely at all. I might not even exhale when I'm walking past you. I don't think masks do crap in this kind of situation. They're just a display.7 -
Interview with an epidemiologist about the mask topic: https://www.ucsf.edu/news/2020/06/417906/still-confused-about-masks-heres-science-behind-how-face-masks-prevent4
-
ExistingFish wrote: »
Without disputing the conclusion at all**, I'd observe that the research is influenza research. Is Covid transmitted identically (same droplet size needed in exhalates for transmission, and that sort of thing), same volume of virus bits needed to infect, same effect of environmentals (heat, light, airflow) on life of virus or other aspects that make it more/less contagious via exhalation, etc.?
I have no idea. Could be identical. Could be not identical. Just because it's a symptomatically similar disease, doesn't make the different virus have the same transmission characteristics, AFAIK.
I didn't link it because it was symptomatically similar, I did because it was a respiratory spread virus - not a bacteria (a previous thing posted was a guy looking at bacteria coming past a mask/not ) - I thought a meta-analysis of influenza spread that was on actual people getting actually ill was far closer to what you'd see with another respiratory virus.
I think masks help some, we've had some people sick, like a hairdresser, who saw customers and didn't spread it to them because they wore masks. That kind of one-on-one close contact? Yeah, I think masks will minimize that. Dentists? Yep.
Me walking down a 10ft wide aisle in a grocery store and passing you for 5 seconds without a mask? Not likely at all. I might not even exhale when I'm walking past you. I don't think masks do crap in this kind of situation. They're just a display.
Yeah, the thing is, as someone with lupus who sometimes takes immune-suppressing drugs, I’ve been aware of airborne disease transmission since well before Covid, and I can tell you, people (not you, but all those other people) do exhale when you walk past them. Humans are nasty, nasty things, and 99.9% of the time every single nasty, disease-bearing one of them will cough loudly, mouth wide open, jaw slack, lungs rattling with phlegm, right as I pass. I have had a runner pass me on a trail and sneeze and spatter me right in the flipping EYE. At Walgreens during flu season I feel like I’m playing an old school video game trying to avoid death, since it’s apparently not possible for anyone in this city to keep their germs to themselves.
Masks do the job for all those disgusting excuses for humans whose mommas never taught them to cover their mouths.22 -
More similar? Sure. Same? Dunno.ExistingFish wrote: »
Without disputing the conclusion at all**, I'd observe that the research is influenza research. Is Covid transmitted identically (same droplet size needed in exhalates for transmission, and that sort of thing), same volume of virus bits needed to infect, same effect of environmentals (heat, light, airflow) on life of virus or other aspects that make it more/less contagious via exhalation, etc.?
I have no idea. Could be identical. Could be not identical. Just because it's a symptomatically similar disease, doesn't make the different virus have the same transmission characteristics, AFAIK.
I didn't link it because it was symptomatically similar, I did because it was a respiratory spread virus - not a bacteria (a previous thing posted was a guy looking at bacteria coming past a mask/not ) - I thought a meta-analysis of influenza spread that was on actual people getting actually ill was far closer to what you'd see with another respiratory virus.I think masks help some, we've had some people sick, like a hairdresser, who saw customers and didn't spread it to them because they wore masks. That kind of one-on-one close contact? Yeah, I think masks will minimize that. Dentists? Yep.
Me walking down a 10ft wide aisle in a grocery store and passing you for 5 seconds without a mask? Not likely at all. I might not even exhale when I'm walking past you. I don't think masks do crap in this kind of situation. They're just a display.
So, at the store: If I stop in the aisle to look at something, and someone else stops nearby, does it help then? If I interact with a store employee for a short conversation? If I sneeze? If I see my friend Suzie, and we talk for a few minutes across that aisle?
I just don't see the downside. I don't like mandates, either. I particularly dislike them without exceptions for people who have breathing or other health limitations, even recognizing that there's no way to guarantee people won't lie about that.
If nothing else, the presymptomatic/asymptomatic contagion is worse with Covid than flu. That makes masks more useful, as a practical matter.
We had a chance to go with voluntary compliance. We flippin' s*cked at it. Mandates are next, and they're not going to be conditional on things like how long, on average, it takes to pass someone in a supermarket.
And read the link lemur posted. We're not just looking at "mask mandate" vs. "no mask mandate". As a practical, epidemiological matter, incidence of mass usage affects ability to resume relatively more economic activity. That's a pretty big deal.
Edit: fix quote tags I broke.15 -
ExistingFish wrote: »ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
Without disputing the conclusion at all**, I'd observe that the research is influenza research. Is Covid transmitted identically (same droplet size needed in exhalates for transmission, and that sort of thing), same volume of virus bits needed to infect, same effect of environmentals (heat, light, airflow) on life of virus or other aspects that make it more/less contagious via exhalation, etc.?
I have no idea. Could be identical. Could be not identical. Just because it's a symptomatically similar disease, doesn't make the different virus have the same transmission characteristics, AFAIK.
It does seem to me that some of what had the experts confused and sending mixed messages, certainly at first but to some extent even now, was that research on factors like those I mentioned were just beginning to be to be published for this specific virus.
I'd also observe that there's some sign that countries with high mask adherence had better virus control, generally (possibly not absolutely). That's a correlational thing, so weak evidence . . . but wearing a mask is pretty easy & cheap, so seems worth doing even if there's some mere correlational findings as the justification. (I understand that some people with health issues can have problems wearing masks. I'm talking in general terms about the population.)
From my amateur history of closely reading other health research (breast cancer), it seems to me that preventatives/treatments with generally no negative side-effects will be accepted as part of standard practice/recommendations based on moderately weak evidence; and things that are more likely to cause harm are subjected to higher standards for proof of effectiveness before becoming standard practice. Outside of the health-related minority end-cases, mask wearing is pretty harmless.
** Not because I think it's indisputable, but because I'm not an expert, and I don't feel like researching/disputing today.
I made it clear it was influenza research, we don't have 70 years of covid research to look at, now do we?
I'm fine with it being a "standard practice/recommendation" that is not the same as a mandate with enforcement.
Mandates, and all this mask-wearing hype (when the science is iffy, at best), it causes discrimination against those who don't. Prejudice. Sanctimonious behavior. Racial discrimination (yes, it has happened). When everyone is hyping it up like if you don't do it, you are gonna kill your grandma - well the science just isn't there.
I'm tired of seeing leaders standing up saying "WEAR YOUR MASKS" and then when they think the camera cuts off, they take it off - if they don't believe it, why are they preaching it? or reporters on the beach saying "No one is wearing masks! The horror!" and a passerby points out their camera guy isn't wearing a mask. It's just becoming a way to point fingers and shame people.
Just a terminology clarification: "Standard practice" in cancer treatment (i.e., standard of care) is not the same as a loosey-goosey voluntary guideline. It's essentially binding on practitioners (i.e., simplistically, it's malpractice to do otherwise, and at extremes there can be legal sanctions). (Patients can opt out, of course. And mask objectors can - frankly - stay home.)
We disagree about the state of the science. I share your concern about discrimination. Shaming is one way desirable social change happens: I'm not always against it. Hypocrites are not a counter-argument.
Though I rarely act out over it, I'm routinely prejudiced against aggressively rude people (in many contexts, not just this one), and - absent medical reasons for it - that's what non-mask-wearers are doing at this point, being aggressively rude. (No, being rude isn't illegal . . . up to a certain point, anyway.)5 -
Interview with an epidemiologist about the mask topic: https://www.ucsf.edu/news/2020/06/417906/still-confused-about-masks-heres-science-behind-how-face-masks-prevent
It's nice. It's a single epidemiologist though, not a study. I read the study linked. It supported the use of masks, as do I. It did not support the use of mandates, which I don't either.
It also said 80% adherence would be enough, so I again, don't think mandates are the answer. I'm fine with suggestion and recommendation. I support that. That is what my state is doing. I wear a mask where required, but I don't think poorly of those who don't. I don't think they are engaging in risky behavior.
The fear and prejudiced feelings about these things are why people are coughing on babies.0 -
ExistingFish wrote: »T1DCarnivoreRunner wrote: »ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
I'm not sure it's the same as influenza. We know Coronavirus is spread by droplets leaving our mouth and nose, so it is logical that a mask that limits droplets will work. Is it 100%? Nope. Nobody ever said it is... but any effectiveness is worthwhile.
In fact, unless if a mask was proven to be 0% effective (not against influenza), they should be required. Even a 1% decrease in spread means more than a thousand lives saved here in the U.S. alone... so far. If you believe your personal convenience is more important than more than 1,000 lives; then just stay home.
Can you point me in the direction of the current death rate? Google seems to be failing me. I came up with 0.04%, this is all deaths - not taking into account comorbidities and stuff. I'm sure an expert could get me a better number. I'm not sure a 1% or 5% effectiveness rate would be worth mandates or enforcement. Would you take a vaccine with a 1% effectiveness rate?
People die in car crashes every year, should we make more restrictive mandates (10mph speed limits) and spend money on enforcement? It would save significantly more people from death or injury.
Don't get me wrong, I wear a mask where required. My state hasn't made a mandate and I'm glad they haven't. They've done contact tracing, people aren't picking up COVID from the gym or the restaurants. The new cases haven't gotten them there. They are getting them from their household, or from large gatherings I'm guessing where social distancing isn't enforced - like protests and other large gatherings.
Are you seriously arguing it is ok for people to die for your convenience?! Seems selfish to me.6 -
T1DCarnivoreRunner wrote: »ExistingFish wrote: »T1DCarnivoreRunner wrote: »ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
I'm not sure it's the same as influenza. We know Coronavirus is spread by droplets leaving our mouth and nose, so it is logical that a mask that limits droplets will work. Is it 100%? Nope. Nobody ever said it is... but any effectiveness is worthwhile.
In fact, unless if a mask was proven to be 0% effective (not against influenza), they should be required. Even a 1% decrease in spread means more than a thousand lives saved here in the U.S. alone... so far. If you believe your personal convenience is more important than more than 1,000 lives; then just stay home.
Can you point me in the direction of the current death rate? Google seems to be failing me. I came up with 0.04%, this is all deaths - not taking into account comorbidities and stuff. I'm sure an expert could get me a better number. I'm not sure a 1% or 5% effectiveness rate would be worth mandates or enforcement. Would you take a vaccine with a 1% effectiveness rate?
People die in car crashes every year, should we make more restrictive mandates (10mph speed limits) and spend money on enforcement? It would save significantly more people from death or injury.
Don't get me wrong, I wear a mask where required. My state hasn't made a mandate and I'm glad they haven't. They've done contact tracing, people aren't picking up COVID from the gym or the restaurants. The new cases haven't gotten them there. They are getting them from their household, or from large gatherings I'm guessing where social distancing isn't enforced - like protests and other large gatherings.
Are you seriously arguing it is ok for people to die for your convenience?! Seems selfish to me.
Fear and feelings aside, we make those kinds of arguments every day. Do you know how many people die or are injured in car crashes? Do you know what decisions they have to make when they set speed limits? They know changing the limit by 5 or 10 mph saves or risks lives. They have to make that kind of decision because people have to go to places.
I don't think it's okay for people to die for my convenience, I never said that and I don't think anything I said should make you arrive at that conclusion. I'm just trying to get you to consider that these kinds of choices are made every day. Should I never get in a car and drive because there is a risk I could hit someone? No, I follow the rules and have insurance, but I take that risk to drive - as does everyone else on the road.
If I thought it was okay for people to die for my convenience, I wouldn't stop at stop signs - that's inconvenient! Who cares if I hit someone. But I do stop, because I do care.
I care about the possibility of spreading covid. I step back and allow people to walk through doorways so we aren't in it together, I stand on the 6' markings when standing in line. I don't shake hands. I use hand sanitizer when entering and leaving stores. I am okay with wearing a mask, but I don't think it is really doing anything when I wear it. I have barely been within 6' of someone for more than 15 seconds (you know, in passing). I don't think that casual contact is enough to spread covid, and from what I've heard, it isn't.4 -
The fear and prejudiced feelings about these things are why people are coughing on babies
Oh, c'mon.
Personality disorders are why people are coughing on babies.
I decided early on that it is none of my business what other people do so I'm not about to point out to a stranger that they need to step back six feet. Instead, I take a large shopping cart and try to keep it between me and the person behind me. There is only so much I can do against sociopathic behavior so since I'm old I try very hard not to put myself in situations that will cause conflict. So far in the past four months no one has gotten mad at me.
16 -
ExistingFish wrote: »Interview with an epidemiologist about the mask topic: https://www.ucsf.edu/news/2020/06/417906/still-confused-about-masks-heres-science-behind-how-face-masks-prevent
It's nice. It's a single epidemiologist though, not a study. I read the study linked. It supported the use of masks, as do I. It did not support the use of mandates, which I don't either.
It also said 80% adherence would be enough, so I again, don't think mandates are the answer. I'm fine with suggestion and recommendation. I support that. That is what my state is doing. I wear a mask where required, but I don't think poorly of those who don't. I don't think they are engaging in risky behavior.
The fear and prejudiced feelings about these things are why people are coughing on babies.
If requirements to wear a mask make a person cough on a baby during a pandemic, there was something wrong with that person long before covid.
Based on what I've seen, many places in the US won't reach 80% compliance without a mandate.
With all the crazy *kitten* people believe without a shred of evidence, I'm fascinated by the amount of people who are now insisting on years of peer reviewed studies about masks. I actually saw someone on FB complain there's not enough science to support wearing a mask, then posted a meme about how they'll kill you by causing you to breathe back in too much CO2.
I've seen enough introductory science and anecdotal evidence to do something that is barely an inconvenience with the hope that it's helping. And I'm legit confused why with all the crazy rules and regulations and power grabs we sleepwalk through everyday, masks in a pandemic is where people would draw the line. <shrug>12 -
cmriverside wrote: »The fear and prejudiced feelings about these things are why people are coughing on babies
Oh, c'mon.
Personality disorders are why people are coughing on babies.
I decided early on that it is none of my business what other people do so I'm not about to point out to a stranger that they need to step back six feet. Instead, I take a large shopping cart and try to keep it between me and the person behind me. There is only so much I can do against sociopathic behavior so since I'm old I try very hard not to put myself in situations that will cause conflict. So far in the past four months no one has gotten mad at me.
Apparently, she worked in the local school district. No one has gotten mad at me, I just see what I consider irrational behavior online.
I'm just watching our state's daily covid update. They did a survey - which I understand isn't scientific or anything - but 82% of respondents say they are wearing masks when they go out. They even broke it down by age. 16% said No, and 2% weren't sure. That's over the 80% that would be needed to slow down covid.
We don't have a mandate. By suggestion and recommendation, we have 84%. No enforcement measures.0 -
ExistingFish wrote: »T1DCarnivoreRunner wrote: »ExistingFish wrote: »T1DCarnivoreRunner wrote: »ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
I'm not sure it's the same as influenza. We know Coronavirus is spread by droplets leaving our mouth and nose, so it is logical that a mask that limits droplets will work. Is it 100%? Nope. Nobody ever said it is... but any effectiveness is worthwhile.
In fact, unless if a mask was proven to be 0% effective (not against influenza), they should be required. Even a 1% decrease in spread means more than a thousand lives saved here in the U.S. alone... so far. If you believe your personal convenience is more important than more than 1,000 lives; then just stay home.
Can you point me in the direction of the current death rate? Google seems to be failing me. I came up with 0.04%, this is all deaths - not taking into account comorbidities and stuff. I'm sure an expert could get me a better number. I'm not sure a 1% or 5% effectiveness rate would be worth mandates or enforcement. Would you take a vaccine with a 1% effectiveness rate?
People die in car crashes every year, should we make more restrictive mandates (10mph speed limits) and spend money on enforcement? It would save significantly more people from death or injury.
Don't get me wrong, I wear a mask where required. My state hasn't made a mandate and I'm glad they haven't. They've done contact tracing, people aren't picking up COVID from the gym or the restaurants. The new cases haven't gotten them there. They are getting them from their household, or from large gatherings I'm guessing where social distancing isn't enforced - like protests and other large gatherings.
Are you seriously arguing it is ok for people to die for your convenience?! Seems selfish to me.
Fear and feelings aside, we make those kinds of arguments every day. Do you know how many people die or are injured in car crashes? Do you know what decisions they have to make when they set speed limits? They know changing the limit by 5 or 10 mph saves or risks lives. They have to make that kind of decision because people have to go to places.
I don't think it's okay for people to die for my convenience, I never said that and I don't think anything I said should make you arrive at that conclusion. I'm just trying to get you to consider that these kinds of choices are made every day. Should I never get in a car and drive because there is a risk I could hit someone? No, I follow the rules and have insurance, but I take that risk to drive - as does everyone else on the road.
If I thought it was okay for people to die for my convenience, I wouldn't stop at stop signs - that's inconvenient! Who cares if I hit someone. But I do stop, because I do care.
I care about the possibility of spreading covid. I step back and allow people to walk through doorways so we aren't in it together, I stand on the 6' markings when standing in line. I don't shake hands. I use hand sanitizer when entering and leaving stores. I am okay with wearing a mask, but I don't think it is really doing anything when I wear it. I have barely been within 6' of someone for more than 15 seconds (you know, in passing). I don't think that casual contact is enough to spread covid, and from what I've heard, it isn't.
Vehicles are used in a lot of ways that are extremely valuable - in fact, in ways that quite literally preserve and save lives. How is the benefit of operating a vehicle the same as the benefit of refusing to wear a mask? This is the part I can't understand about anti-maskers. I understand the benefits of wearing a mask. I have yet to hear more than "cuz muh freedoms..." or "I don't like the way it looks / feels" as a reason to not wear a mask.14 -
rheddmobile wrote: »ExistingFish wrote: »
Without disputing the conclusion at all**, I'd observe that the research is influenza research. Is Covid transmitted identically (same droplet size needed in exhalates for transmission, and that sort of thing), same volume of virus bits needed to infect, same effect of environmentals (heat, light, airflow) on life of virus or other aspects that make it more/less contagious via exhalation, etc.?
I have no idea. Could be identical. Could be not identical. Just because it's a symptomatically similar disease, doesn't make the different virus have the same transmission characteristics, AFAIK.
I didn't link it because it was symptomatically similar, I did because it was a respiratory spread virus - not a bacteria (a previous thing posted was a guy looking at bacteria coming past a mask/not ) - I thought a meta-analysis of influenza spread that was on actual people getting actually ill was far closer to what you'd see with another respiratory virus.
I think masks help some, we've had some people sick, like a hairdresser, who saw customers and didn't spread it to them because they wore masks. That kind of one-on-one close contact? Yeah, I think masks will minimize that. Dentists? Yep.
Me walking down a 10ft wide aisle in a grocery store and passing you for 5 seconds without a mask? Not likely at all. I might not even exhale when I'm walking past you. I don't think masks do crap in this kind of situation. They're just a display.
Yeah, the thing is, as someone with lupus who sometimes takes immune-suppressing drugs, I’ve been aware of airborne disease transmission since well before Covid, and I can tell you, people (not you, but all those other people) do exhale when you walk past them. Humans are nasty, nasty things, and 99.9% of the time every single nasty, disease-bearing one of them will cough loudly, mouth wide open, jaw slack, lungs rattling with phlegm, right as I pass. I have had a runner pass me on a trail and sneeze and spatter me right in the flipping EYE. At Walgreens during flu season I feel like I’m playing an old school video game trying to avoid death, since it’s apparently not possible for anyone in this city to keep their germs to themselves.
Masks do the job for all those disgusting excuses for humans whose mommas never taught them to cover their mouths.
My dad died many years ago; he lived to be 90. On one of our trips to the ER with him, I can distinctly remember passing a woman who happened to cough right as we walked by; the timing completely sucked. My thought was ohno , I hope he doesn't end up sick from that 3 second pass-by coughing that was unprotected by all of us. My dad ended up in the VA hospital for a week, with pneumonia. That's how quick and easily germs can pass with no barriers. 17 -
T1DCarnivoreRunner wrote: »ExistingFish wrote: »T1DCarnivoreRunner wrote: »ExistingFish wrote: »T1DCarnivoreRunner wrote: »ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
I'm not sure it's the same as influenza. We know Coronavirus is spread by droplets leaving our mouth and nose, so it is logical that a mask that limits droplets will work. Is it 100%? Nope. Nobody ever said it is... but any effectiveness is worthwhile.
In fact, unless if a mask was proven to be 0% effective (not against influenza), they should be required. Even a 1% decrease in spread means more than a thousand lives saved here in the U.S. alone... so far. If you believe your personal convenience is more important than more than 1,000 lives; then just stay home.
Can you point me in the direction of the current death rate? Google seems to be failing me. I came up with 0.04%, this is all deaths - not taking into account comorbidities and stuff. I'm sure an expert could get me a better number. I'm not sure a 1% or 5% effectiveness rate would be worth mandates or enforcement. Would you take a vaccine with a 1% effectiveness rate?
People die in car crashes every year, should we make more restrictive mandates (10mph speed limits) and spend money on enforcement? It would save significantly more people from death or injury.
Don't get me wrong, I wear a mask where required. My state hasn't made a mandate and I'm glad they haven't. They've done contact tracing, people aren't picking up COVID from the gym or the restaurants. The new cases haven't gotten them there. They are getting them from their household, or from large gatherings I'm guessing where social distancing isn't enforced - like protests and other large gatherings.
Are you seriously arguing it is ok for people to die for your convenience?! Seems selfish to me.
Fear and feelings aside, we make those kinds of arguments every day. Do you know how many people die or are injured in car crashes? Do you know what decisions they have to make when they set speed limits? They know changing the limit by 5 or 10 mph saves or risks lives. They have to make that kind of decision because people have to go to places.
I don't think it's okay for people to die for my convenience, I never said that and I don't think anything I said should make you arrive at that conclusion. I'm just trying to get you to consider that these kinds of choices are made every day. Should I never get in a car and drive because there is a risk I could hit someone? No, I follow the rules and have insurance, but I take that risk to drive - as does everyone else on the road.
If I thought it was okay for people to die for my convenience, I wouldn't stop at stop signs - that's inconvenient! Who cares if I hit someone. But I do stop, because I do care.
I care about the possibility of spreading covid. I step back and allow people to walk through doorways so we aren't in it together, I stand on the 6' markings when standing in line. I don't shake hands. I use hand sanitizer when entering and leaving stores. I am okay with wearing a mask, but I don't think it is really doing anything when I wear it. I have barely been within 6' of someone for more than 15 seconds (you know, in passing). I don't think that casual contact is enough to spread covid, and from what I've heard, it isn't.
Vehicles are used in a lot of ways that are extremely valuable - in fact, in ways that quite literally preserve and save lives. How is the benefit of operating a vehicle the same as the benefit of refusing to wear a mask? This is the part I can't understand about anti-maskers. I understand the benefits of wearing a mask. I have yet to hear more than "cuz muh freedoms..." or "I don't like the way it looks / feels" as a reason to not wear a mask.
I never said I was against masks, I'm against mandates that require enforcement. That takes law enforcement or regulators away from things where they are really needed. I don't want our already stressed first responders coming to dispute with individuals about mask-wearing. That does cost. That opens them for more discrimination issues that they are already facing. You can't just say "oh we should mandate that!" it costs businesses, it requires law enforcement (at the same time everyone is calling for defunding and disbandment of law enforcement)
All this and Governor is now allowing cities to mandate (city by city) mask-wearing.1 -
ExistingFish wrote: »ExistingFish wrote: »ExistingFish wrote: »https://wwwnc.cdc.gov/eid/article/26/5/19-0994_article
This article is about influenza, but influenza is very much like covid in the fact that it is a contagious respiratory disease.
Thoughts?
I'm really interested to hear the opinions on those who want to mandate face masks:
Face Mask
In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018. In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks (RR 0.78, 95% CI 0.51–1.20; I2 = 30%, p = 0.25) (Figure 2). One study evaluated the use of masks among pilgrims from Australia during the Hajj pilgrimage and reported no major difference in the risk for laboratory-confirmed influenza virus infection in the control or mask group (33). Two studies in university settings assessed the effectiveness of face masks for primary protection by monitoring the incidence of laboratory-confirmed influenza among student hall residents for 5 months (9,10). The overall reduction in ILI or laboratory-confirmed influenza cases in the face mask group was not significant in either studies (9,10). Study designs in the 7 household studies were slightly different: 1 study provided face masks and P2 respirators for household contacts only (34), another study evaluated face mask use as a source control for infected persons only (35), and the remaining studies provided masks for the infected persons as well as their close contacts (11–13,15,17). None of the household studies reported a significant reduction in secondary laboratory-confirmed influenza virus infections in the face mask group (11–13,15,17,34,35). Most studies were underpowered because of limited sample size, and some studies also reported suboptimal adherence in the face mask group.
Disposable medical masks (also known as surgical masks) are loose-fitting devices that were designed to be worn by medical personnel to protect accidental contamination of patient wounds, and to protect the wearer against splashes or sprays of bodily fluids (36). There is limited evidence for their effectiveness in preventing influenza virus transmission either when worn by the infected person for source control or when worn by uninfected persons to reduce exposure. Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza.
Without disputing the conclusion at all**, I'd observe that the research is influenza research. Is Covid transmitted identically (same droplet size needed in exhalates for transmission, and that sort of thing), same volume of virus bits needed to infect, same effect of environmentals (heat, light, airflow) on life of virus or other aspects that make it more/less contagious via exhalation, etc.?
I have no idea. Could be identical. Could be not identical. Just because it's a symptomatically similar disease, doesn't make the different virus have the same transmission characteristics, AFAIK.
It does seem to me that some of what had the experts confused and sending mixed messages, certainly at first but to some extent even now, was that research on factors like those I mentioned were just beginning to be to be published for this specific virus.
I'd also observe that there's some sign that countries with high mask adherence had better virus control, generally (possibly not absolutely). That's a correlational thing, so weak evidence . . . but wearing a mask is pretty easy & cheap, so seems worth doing even if there's some mere correlational findings as the justification. (I understand that some people with health issues can have problems wearing masks. I'm talking in general terms about the population.)
From my amateur history of closely reading other health research (breast cancer), it seems to me that preventatives/treatments with generally no negative side-effects will be accepted as part of standard practice/recommendations based on moderately weak evidence; and things that are more likely to cause harm are subjected to higher standards for proof of effectiveness before becoming standard practice. Outside of the health-related minority end-cases, mask wearing is pretty harmless.
** Not because I think it's indisputable, but because I'm not an expert, and I don't feel like researching/disputing today.
I made it clear it was influenza research, we don't have 70 years of covid research to look at, now do we?
I'm fine with it being a "standard practice/recommendation" that is not the same as a mandate with enforcement.
Mandates, and all this mask-wearing hype (when the science is iffy, at best), it causes discrimination against those who don't. Prejudice. Sanctimonious behavior. Racial discrimination (yes, it has happened). When everyone is hyping it up like if you don't do it, you are gonna kill your grandma - well the science just isn't there.
I'm tired of seeing leaders standing up saying "WEAR YOUR MASKS" and then when they think the camera cuts off, they take it off - if they don't believe it, why are they preaching it? or reporters on the beach saying "No one is wearing masks! The horror!" and a passerby points out their camera guy isn't wearing a mask. It's just becoming a way to point fingers and shame people.
@ExistingFish what state are you in?
I'm in MA, where we've had local mask mandates and then a state mandate for some time.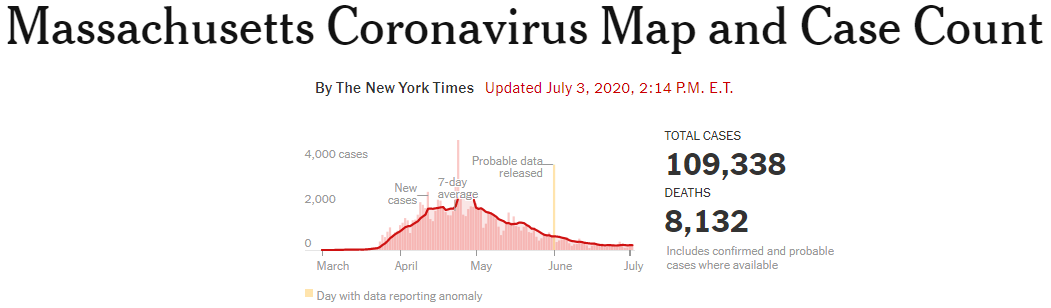 7
7 -
Where I live, we have a Sheriff, a Deputy, and one Patrol Officer. I don't think having them running around mandating masks is a good use of their time.2
-
ExistingFish wrote: »cmriverside wrote: »The fear and prejudiced feelings about these things are why people are coughing on babies
Oh, c'mon.
Personality disorders are why people are coughing on babies.
I decided early on that it is none of my business what other people do so I'm not about to point out to a stranger that they need to step back six feet. Instead, I take a large shopping cart and try to keep it between me and the person behind me. There is only so much I can do against sociopathic behavior so since I'm old I try very hard not to put myself in situations that will cause conflict. So far in the past four months no one has gotten mad at me.
Apparently, she worked in the local school district. No one has gotten mad at me, I just see what I consider irrational behavior online.
I'm just watching our state's daily covid update. They did a survey - which I understand isn't scientific or anything - but 82% of respondents say they are wearing masks when they go out. They even broke it down by age. 16% said No, and 2% weren't sure. That's over the 80% that would be needed to slow down covid.
We don't have a mandate. By suggestion and recommendation, we have 84%. No enforcement measures.
This survey? https://www.ipsos.com/sites/default/files/ct/news/documents/2020-06/topline-axios-poll-wave-14.pdf
I live in TN - the lowest rate of any of the states included in results - and my observation is that we are nowhere near the level who said they wear a mask. But that also depends on location. My work requires it and I'm almost certain everyone in my dept. is going to claim "yes" as to wearing a mask. I'm also certain they don't wear a mask when outside of work, especially since half of the people in my dept. have expressed their opposition to wearing masks in stores. The rate found for my state is minimum 3 times higher than reality and likely closer to 7-8 times higher than reality, but I'm being very conservative to average out for places like Memphis and Nashville. Note the survey was taken before Memphis' mask ordinance took effect, so hopefully better now (but still not enough).3 -
T1DCarnivoreRunner wrote: »ExistingFish wrote: »cmriverside wrote: »The fear and prejudiced feelings about these things are why people are coughing on babies
Oh, c'mon.
Personality disorders are why people are coughing on babies.
I decided early on that it is none of my business what other people do so I'm not about to point out to a stranger that they need to step back six feet. Instead, I take a large shopping cart and try to keep it between me and the person behind me. There is only so much I can do against sociopathic behavior so since I'm old I try very hard not to put myself in situations that will cause conflict. So far in the past four months no one has gotten mad at me.
Apparently, she worked in the local school district. No one has gotten mad at me, I just see what I consider irrational behavior online.
I'm just watching our state's daily covid update. They did a survey - which I understand isn't scientific or anything - but 82% of respondents say they are wearing masks when they go out. They even broke it down by age. 16% said No, and 2% weren't sure. That's over the 80% that would be needed to slow down covid.
We don't have a mandate. By suggestion and recommendation, we have 84%. No enforcement measures.
This survey? https://www.ipsos.com/sites/default/files/ct/news/documents/2020-06/topline-axios-poll-wave-14.pdf
I live in TN - the lowest rate of any of the states included in results - and my observation is that we are nowhere near the level who said they wear a mask. But that also depends on location. My work requires it and I'm almost certain everyone in my dept. is going to claim "yes" as to wearing a mask. I'm also certain they don't wear a mask when outside of work, especially since half of the people in my dept. have expressed their opposition to wearing masks in stores. The rate found for my state is minimum 3 times higher than reality and likely closer to 7-8 times higher than reality, but I'm being very conservative to average out for places like Memphis and Nashville. Note the survey was taken before Memphis' mask ordinance took effect, so hopefully better now (but still not enough).
In my experience, I would say 75-85% wear masks, which is pretty close to the slides he showed. Your link didn't load for me.0









Categories
- All Categories
- 1.4M Health, Wellness and Goals
- 398.3K Introduce Yourself
- 44.7K Getting Started
- 261K Health and Weight Loss
- 176.4K Food and Nutrition
- 47.7K Recipes
- 233K Fitness and Exercise
- 462 Sleep, Mindfulness and Overall Wellness
- 6.5K Goal: Maintaining Weight
- 8.7K Goal: Gaining Weight and Body Building
- 153.5K Motivation and Support
- 8.4K Challenges
- 1.4K Debate Club
- 96.5K Chit-Chat
- 2.6K Fun and Games
- 4.7K MyFitnessPal Information
- 17 News and Announcements
- 21 MyFitnessPal Academy
- 1.5K Feature Suggestions and Ideas
- 3.2K MyFitnessPal Tech Support Questions